

Significant modification of traditional rapid sequence induction improves safety and effectiveness of pre-hospital trauma anaesthesia
- PMID: 25879683
- PMCID: PMC4391675
- DOI: 10.1186/s13054-015-0872-2
Significant modification of traditional rapid sequence induction improves safety and effectiveness of pre-hospital trauma anaesthesia
Abstract
Introduction: Rapid Sequence Induction of anaesthesia (RSI) is the recommended method to facilitate emergency tracheal intubation in trauma patients. In emergency situations, a simple and standardised RSI protocol may improve the safety and effectiveness of the procedure. A crucial component of developing a standardised protocol is the selection of induction agents. The aim of this study is to compare the safety and effectiveness of a traditional RSI protocol using etomidate and suxamethonium with a modified RSI protocol using fentanyl, ketamine and rocuronium.
Methods: We performed a comparative cohort study of major trauma patients undergoing pre-hospital RSI by a physician-led Helicopter Emergency Medical Service. Group 1 underwent RSI using etomidate and suxamethonium and Group 2 underwent RSI using fentanyl, ketamine and rocuronium. Apart from the induction agents, the RSI protocol was identical in both groups. Outcomes measured included laryngoscopy view, intubation success, haemodynamic response to laryngoscopy and tracheal intubation, and mortality.
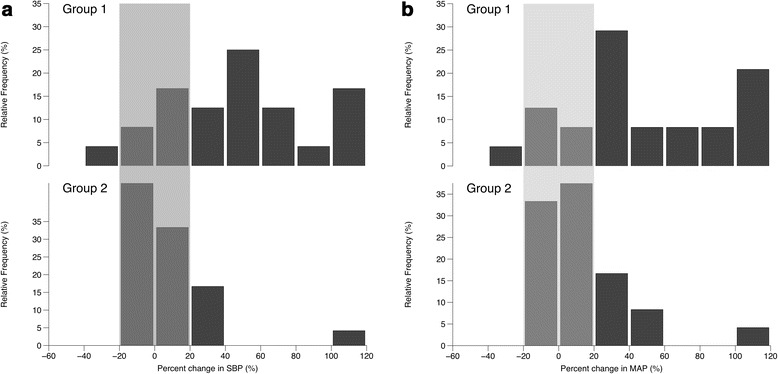
Results: Compared to Group 1 (n = 116), Group 2 RSI (n = 145) produced significantly better laryngoscopy views (p = 0.013) and resulted in significantly higher first-pass intubation success (95% versus 100%; p = 0.007). A hypertensive response to laryngoscopy and tracheal intubation was less frequent following Group 2 RSI (79% versus 37%; p < 0.0001). A hypotensive response was uncommon in both groups (1% versus 6%; p = 0.05). Only one patient in each group developed true hypotension (SBP < 90 mmHg) on induction.
Conclusions: In a comparative, cohort study, pre-hospital RSI using fentanyl, ketamine and rocuronium produced superior intubating conditions and a more favourable haemodynamic response to laryngoscopy and tracheal intubation. An RSI protocol using fixed ratios of these agents delivers effective pre-hospital trauma anaesthesia.
Figures



References
-
- Wallace C, McGuire B. Rapid sequence induction: its place in modern anaesthesia. Contin Educ Anaesthesia Crit Care Pain. 2014;14:130–5. doi: 10.1093/bjaceaccp/mkt047. - DOI
-
- The Association of Anaesthetists of Great Britain and Ireland. Pre-hospital Anaesthesia: A safety guideline. http://www.asgbi.org/sites/default/files/prehospital_glossy09.pdf (2009). Accessed 17 August 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
