

Takayasu arteritis in childhood: retrospective experience from a tertiary referral centre in the United Kingdom
- PMID: 25879697
- PMCID: PMC4392477
- DOI: 10.1186/s13075-015-0545-1
Takayasu arteritis in childhood: retrospective experience from a tertiary referral centre in the United Kingdom
Abstract
Introduction: Takayasu arteritis (TA) is an idiopathic large-vessel vasculitis affecting the aorta and its major branches. Although the disease rarely affects children, it does occur, even in infants. The objective of this study was to evaluate the clinical features, disease activity, treatment and outcome of childhood TA in a tertiary UK centre.
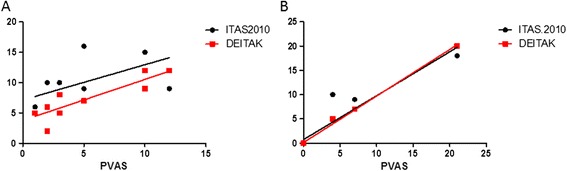
Methods: We analysed a retrospective case series of children fulfilling the TA classification criteria of the European League against Rheumatism, the Paediatric Rheumatology European Society and the Paediatric Rheumatology International Trials Organisation. Data regarding demographics, clinical features, treatments and outcomes were recorded. Descriptive statistics are expressed as median and range. Fisher's exact test was used for group comparisons. The Paediatric Vasculitis Activity Score (PVAS), Paediatric Vasculitis Damage Index (PVDI), Disease Extent Index-Takayasu (DEI.Tak) and Indian Takayasu Arteritis Activity Score (ITAS2010) were calculated retrospectively.
Results: A total of 11 children (64% female) with age at diagnosis of 11.8 (1.3 to 17) years were identified over a 23-year period. The median time to diagnosis was 17 (0 to 132) months. The most common clinical features at presentation were arterial hypertension (72.7%), systemic features (36%) and cardiovascular (45%), neurological (36%), pulmonary (27%), skin (9%), renal (9%) and gastrointestinal (9%) involvement. At presentation, PVAS was 5/63 (1 to 13); DEI.Tak was 7/81 (2 to 12) and ITAS2010 was 9/57 (6 to 20). Treatment included corticosteroids (81.8%), combined with methotrexate in most cases (72.7%). Cyclophosphamide (36.4%) and biologic agents (45.5%) were reserved for severe and/or refractory cases. PVDI at latest follow-up was 5.5/72 (3 to 15). Mortality was 27%. Young age at disease onset (<5 years old) and permanent PVDI scores≥3 were significantly associated with mortality risk (P=0.024).
Conclusion: TA is a rare and potentially life-threatening large-vessel vasculitis. Improved awareness of TA is essential to secure a timely diagnosis. Although the evidence base for the treatment of TA in children is weak, we found that it is essential to treat it aggressively because our data emphasise that the mortality and morbidity in the paediatric population remains high.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
