

Variable performance of models for predicting methicillin-resistant Staphylococcus aureus carriage in European surgical wards
- PMID: 25880328
- PMCID: PMC4347652
- DOI: 10.1186/s12879-015-0834-y
Variable performance of models for predicting methicillin-resistant Staphylococcus aureus carriage in European surgical wards
Abstract
Background: Predictive models to identify unknown methicillin-resistant Staphylococcus aureus (MRSA) carriage on admission may optimise targeted MRSA screening and efficient use of resources. However, common approaches to model selection can result in overconfident estimates and poor predictive performance. We aimed to compare the performance of various models to predict previously unknown MRSA carriage on admission to surgical wards.
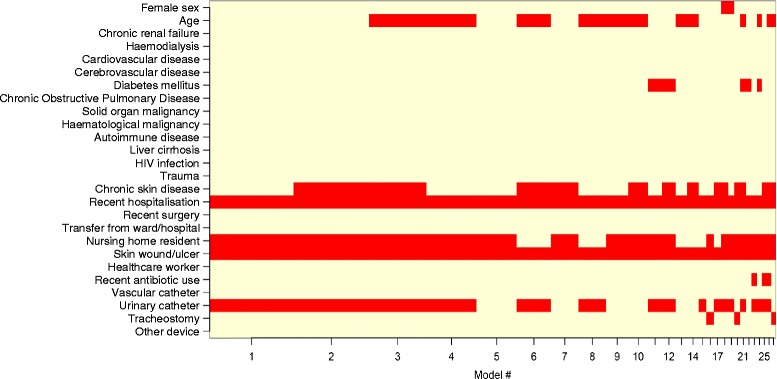
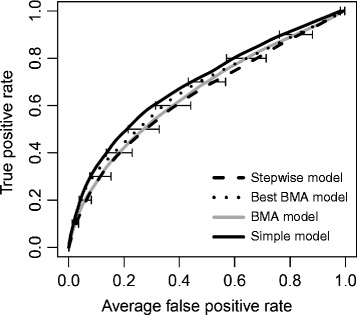
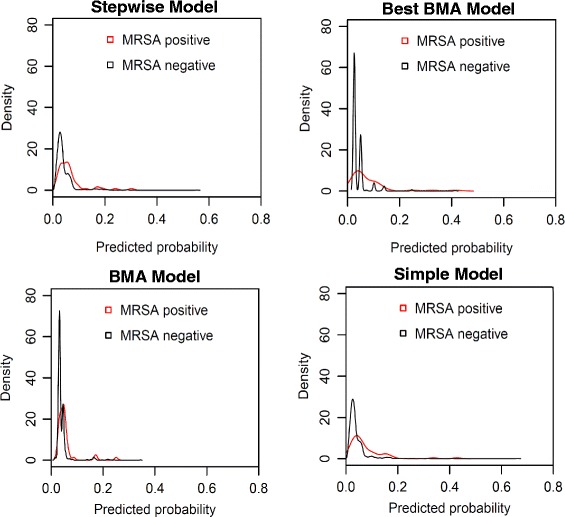
Methods: The study analysed data collected during a prospective cohort study which enrolled consecutive adult patients admitted to 13 surgical wards in 4 European hospitals. The participating hospitals were located in Athens (Greece), Barcelona (Spain), Cremona (Italy) and Paris (France). Universal admission MRSA screening was performed in the surgical wards. Data regarding demographic characteristics and potential risk factors for MRSA carriage were prospectively collected during the study period. Four logistic regression models were used to predict probabilities of unknown MRSA carriage using risk factor data: "Stepwise" (variables selected by backward elimination); "Best BMA" (model with highest posterior probability using Bayesian model averaging which accounts for uncertainty in model choice); "BMA" (average of all models selected with BMA); and "Simple" (model including variables selected >50% of the time by both Stepwise and BMA approaches applied to repeated random sub-samples of 50% of the data). To assess model performance, cross-validation against data not used for model fitting was conducted and net reclassification improvement (NRI) was calculated.
Results: Of 2,901 patients enrolled, 111 (3.8%) were newly identified MRSA carriers. Recent hospitalisation and presence of a wound/ulcer were significantly associated with MRSA carriage in all models. While all models demonstrated limited predictive ability (mean c-statistics <0.7) the Simple model consistently detected more MRSA-positive individuals despite screening fewer patients than the Stepwise model. Moreover, the Simple model improved reclassification of patients into appropriate risk strata compared with the Stepwise model (NRI 6.6%, P = .07).
Conclusions: Though commonly used, models developed using stepwise variable selection can have relatively poor predictive value. When developing MRSA risk indices, simpler models, which account for uncertainty in model selection, may better stratify patients' risk of unknown MRSA carriage.
Figures
References
-
- Weber SG, Huang SS, Oriola S, Huskins WC, Noskin GA, Harriman K, et al. Legislative mandates for use of active surveillance cultures to screen for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci: Position statement from the Joint SHEA and APIC Task Force. Am J Infect Control. 2007;35:73–85. doi: 10.1016/j.ajic.2007.01.001. - DOI - PubMed
-
- UK Department of Health. MRSA Screening - Operational Guidance 2. [http://webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.g...]
-
- Robotham JV, Graves N, Cookson BD, Barnett AG, Wilson JA, Edgeworth JD, et al. Screening, isolation, and decolonisation strategies in the control of meticillin resistant Staphylococcus aureus in intensive care units: cost effectiveness evaluation. BMJ. 2011;343:d5694. doi: 10.1136/bmj.d5694. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
