

Did Medicare Part D reduce disparities?
- PMID: 25880361
- PMCID: PMC4405127
Did Medicare Part D reduce disparities?
Abstract
Objectives: We assessed whether Medicare Part D reduced disparities in access to medication.
Study design: Secondary data analysis of a 20% sample of Medicare beneficiaries, using Parts A and B medical claims from 2002 to 2008 and Part D drug claims from 2006 to 2008.
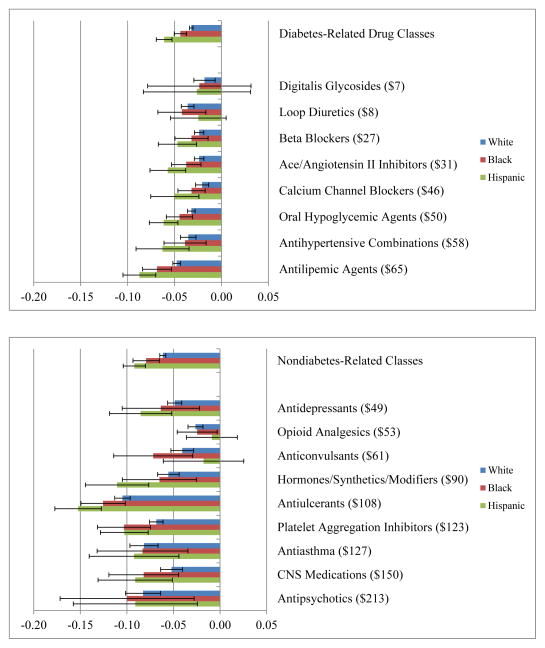
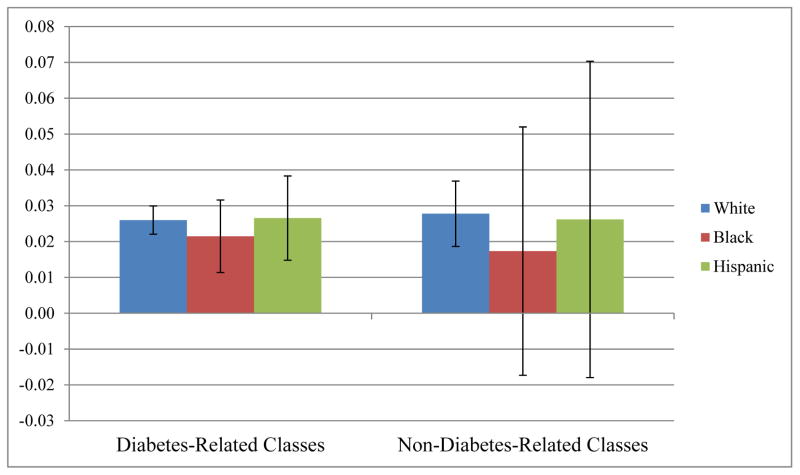
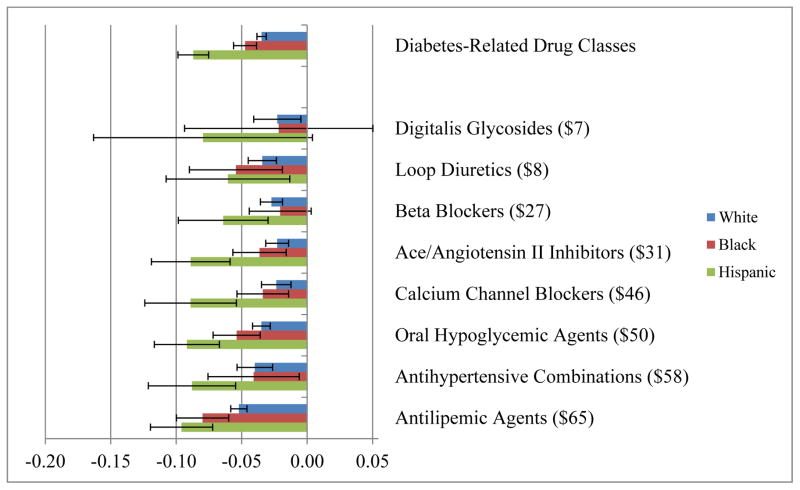
Methods: We analyzed the medication use of Hispanic, black, and white beneficiaries with diabetes before and after reaching the Part D coverage gap, and compared their use with that of race-specific reference groups not exposed to the loss in coverage. Unadjusted difference-in-difference results were validated with multivariate regression models adjusted for demographics, comorbidities, and zip code-level household income used as a proxy for socioeconomic status.
Results: The rate at which Hispanics reduced use of diabetes-related medications in the coverage gap was twice as high as whites, while blacks decreased their use of diabetes-related medications by 33% more than whites. The reduction in medication use was correlated with drug price. Hispanics and blacks were more likely than whites to discontinue a therapy after reaching the coverage gap but more likely to resume once coverage restarted. Hispanics without subsidies and living in low-income areas reduced medication use more than similar blacks and whites in the coverage gap.
Conclusions: We found that the Part D coverage gap is particularly disruptive to minorities and those living in low-income areas. The implications of this work suggest that protecting the health of vulnerable groups requires more than premium subsidies. Patient education may be a first step, but more substantive improvements in adherence may require changes in healthcare delivery.
Conflict of interest statement
Figures
References
-
- KRC Research; KRC Research, editor; KRC Research, translator. Seniors’ Opinions About Medicare Rx: Sixth Year Update. Washington, DC: KRC Research; 2011.
-
- Group TDCaCTR. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. New Engl J Med. 1993;329(14):977–986. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
