

APOE ε4 moderates abnormal CSF-abeta-42 levels, while neurocognitive impairment is associated with abnormal CSF tau levels in HIV+ individuals - a cross-sectional observational study
- PMID: 25880550
- PMCID: PMC4386081
- DOI: 10.1186/s12883-015-0298-0
APOE ε4 moderates abnormal CSF-abeta-42 levels, while neurocognitive impairment is associated with abnormal CSF tau levels in HIV+ individuals - a cross-sectional observational study
Abstract
Background: Cerebrospinal fluid (CSF) biomarkers Aβ1-42, t-tau and p-tau have a characteristic pattern in Alzheimer's Disease (AD). Their roles in HIV-associated neurocognitive disorder (HAND) remains unclear.
Methods: Adults with chronic treated HIV disease were recruited (n = 43, aged 56.7 ± 7.9; 32% aged 60+; median HIV duration 20 years, >95% plasma and CSF HIV RNA <50 cp/mL, on cART for a median 24 months). All underwent standard neuropsychological testing (61% had HAND), APOE genotyping (30.9% carried APOE ε4 and 7.1% were ε4 homozygotes) and a lumbar puncture. Concentrations of Aβ1-42, t-tau and p-tau were assessed in the CSF using commercial ELISAs. Current neurocognitive status was defined using the continuous Global Deficit Score, which grades impairment in clinically relevant categories. History of HAND was recorded. Univariate correlations informed multivariate models, which were corrected for nadir CD4-T cell counts and HIV duration.
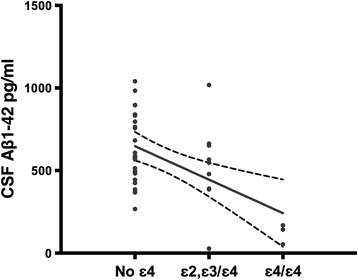
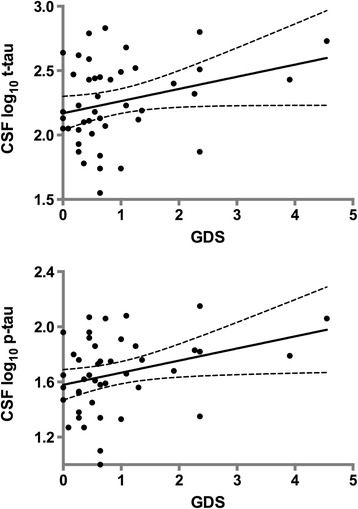
Results: Carriage of APOE ε4 predicted markedly lower levels of CSF Aβ1-42 in univariate (r = -.50; p = .001) and multivariate analyses (R(2) = .25; p < .0003). Greater levels of neurocognitive impairment were associated with higher CSF levels of p-tau in univariate analyses (r = .32; p = .03) and multivariate analyses (R(2) = .10; p = .03). AD risk prediction cut-offs incorporating all three CSF biomarkers suggested that 12.5% of participants had a high risk for AD. Having a CSF-AD like profile was more frequent in those with current (p = .05) and past HIV-associated dementia (p = .03).
Conclusions: Similarly to larger studies, APOE ε4 genotype was not directly associated with HAND, but moderated CSF levels of Aβ1-42 in a minority of participants. In the majority of participants, increased CSF p-tau levels were associated with current neurocognitive impairment. Combined CSF biomarker risk for AD in the current HIV+ sample is more than 10 times greater than in the Australian population of the same age. Larger prospective studies are warranted.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
