

Effect of maternal skin-to-skin contact on decolonization of Methicillin-Oxacillin-Resistant Staphylococcus in neonatal intensive care units: a randomized controlled trial
- PMID: 25880822
- PMCID: PMC4374510
- DOI: 10.1186/s12884-015-0496-1
Effect of maternal skin-to-skin contact on decolonization of Methicillin-Oxacillin-Resistant Staphylococcus in neonatal intensive care units: a randomized controlled trial
Abstract
Background: Decolonization with topical antibiotics is necessary to control outbreaks of multidrug-resistant bacterial infection in the Neonatal Intensive Care Unit (NICU), but can trigger bacterial resistance. The objective of this study was to determine whether skin-to-skin contact of newborns colonized with Methicillin-Oxacillin Resistant Staphylococcus aureus or Methicillin-Oxacillin-Resistant Coagulase-Negative Staphylococcus aureus (MRSA/MRSE) with their mothers could be an effective alternative to promote bacterial decolonization of newborns' nostrils.
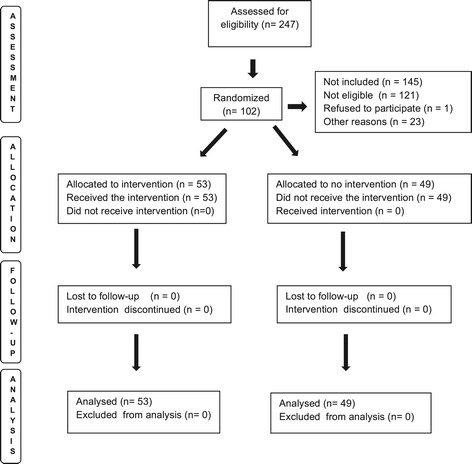
Methods: We performed a randomized clinical trial with 102 newborns admitted to the NICU in three hospitals in São Luís, Brazil. Inclusion criteria were birth weight of 1300 to 1800 g, more than 4 days of hospitalization, newborns with positive nostril cultures for MRSA and/or multidrug-resistant coagulase-negative Staphylococcus and mothers not colonized by these bacteria. We used a random number algorithm for randomization. Allocation was performed using sealed opaque envelopes. Skin-to-skin contact was given twice a day for 60 minutes for seven consecutive days. The control group received routine care without skin-to-skin contact. There was no masking of newborn's mothers or researchers but the individuals who carried out bacterial cultures and assessed results were kept blind to group allocation. The primary outcome was colonization status of newborns' nostrils after 7 days of intervention. The directional hypothesis was that more newborns who receive skin-to-skin holding 2 hours/day for 7 days than newborns who receive normal care will be decolonized.
Results: Decolonization of MRSA/MRSE was greater in the intervention group (Risk Ratio = 2.27; 95% CI 1.27-4.07, p-value = 0.003). Number Needed to Treat (NNT) was 4.0 (95% CI 2.2 - 9.4). After adjustment for the possible confounding effects of small for gestational age birth, antibiotic use, need for resuscitation, sex and cesarean delivery, skin-to-skin contact remained strongly associated with decolonization of newborns' nostrils from MRSA/MRSE bacteria (p = 0.007). There was no need to interrupt the trial for safety reasons.
Conclusion: Skin-to-skin contact might be an effective and safe method for promoting decolonization of newborns' nostrils colonized by MRSA/MRSE.
Trial registration: The study was registered with ClinicalTrials.gov ( NCT01498133 , November 21, 2011).
Figures
Similar articles
-
Emergence of community-associated methicillin-resistant Staphylococcus aureus strains in the neonatal intensive care unit: an infection prevention and patient safety challenge.Clin Microbiol Infect. 2016 Jul;22(7):645.e1-8. doi: 10.1016/j.cmi.2016.04.013. Epub 2016 Apr 25. Clin Microbiol Infect. 2016. PMID: 27126609 Free PMC article.
-
Meticillin-resistant Staphylococcus aureus (MRSA) acquisition risk in an endemic neonatal intensive care unit with an active surveillance culture and decolonization programme.J Hosp Infect. 2017 Jan;95(1):91-97. doi: 10.1016/j.jhin.2016.10.022. Epub 2016 Nov 4. J Hosp Infect. 2017. PMID: 27887754 Free PMC article.
-
Clinical outcomes in methicillin-resistant Staphylococcus aureus-colonized neonates in the neonatal intensive care unit.Neonatology. 2007;91(4):241-7. doi: 10.1159/000098171. Epub 2006 Dec 22. Neonatology. 2007. PMID: 17568155
-
Methicillin-Resistant Staphylococcus aureus Carriage among Neonate Mothers, Healthcare Workers, and Environmental Samples in Neonatal Intensive Care Units: A Systematic Review.Biomed Res Int. 2024 Apr 8;2024:5675786. doi: 10.1155/2024/5675786. eCollection 2024. Biomed Res Int. 2024. PMID: 38623471 Free PMC article.
-
Agents for the decolonization of methicillin-resistant Staphylococcus aureus.Pharmacotherapy. 2009 Mar;29(3):263-80. doi: 10.1592/phco.29.3.263. Pharmacotherapy. 2009. PMID: 19249946 Review.
Cited by
-
Skin-to-skin contact and deaths in newborns weighing up to 1800 grams: a cohort study.J Pediatr (Rio J). 2022 Jul-Aug;98(4):376-382. doi: 10.1016/j.jped.2021.09.001. Epub 2021 Oct 17. J Pediatr (Rio J). 2022. PMID: 34670115 Free PMC article.
-
Early skin-to-skin contact for mothers and their healthy newborn infants.Cochrane Database Syst Rev. 2016 Nov 25;11(11):CD003519. doi: 10.1002/14651858.CD003519.pub4. Cochrane Database Syst Rev. 2016. PMID: 27885658 Free PMC article.
-
Early skin-to-skin contact and risk of late-onset-sepsis in very and extremely preterm infants.Pediatr Res. 2023 Jun;93(7):2091-2100. doi: 10.1038/s41390-022-02383-3. Epub 2022 Nov 14. Pediatr Res. 2023. PMID: 36376509
-
Born Too Soon: Progress and priorities for respectful and rights-based preterm birth care.Reprod Health. 2025 Jun 23;22(Suppl 2):112. doi: 10.1186/s12978-025-02042-w. Reprod Health. 2025. PMID: 40555976 Free PMC article. Review.
-
The role of breast milk in the colonization of neonatal gut and skin with coagulase-negative staphylococci.Pediatr Res. 2017 Nov;82(5):759-767. doi: 10.1038/pr.2017.150. Epub 2017 Aug 2. Pediatr Res. 2017. PMID: 28665928
References
-
- Nelson MU, Bizzarro MJ, Dembry LM, Baltimore RS, Gallagher PG. One size does not fit all: why universal decolonization strategies to prevent methicillin-resistant Staphylococcus aureus colonization and infection in adult intensive care units may be inappropriate for neonatal intensive care units. J Perinatol. 2014;34:653–5. doi: 10.1038/jp.2014.125. - DOI - PMC - PubMed
-
- Gerber SI1, Jones RC, Scott MV, Price JS, Dworkin MS, Filippell MB, Rearick T, Pur SL, McAuley JB, Lavin MA, Welbel SF, Garcia-Houchins S, Bova JL, Weber SG, Arnow PM, Englund JA, Gavin PJ, Fisher AG, Thomson RB, Vescio T, Chou T, Johnson DC, Fry MB, Molloy AH, Bardowski L, Noskin GA. Management of outbreaks of methicillin-resistant Staphylococcus aureus infection in the neonatal intensive care unit: a consensus statement. Infect Control Hosp Epidemiol. 2006;27:139–145. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
