

The relationship between N-terminal prosomatostatin, all-cause and cardiovascular mortality in patients with type 2 diabetes mellitus (ZODIAC-35)
- PMID: 25880900
- PMCID: PMC4404603
- DOI: 10.1186/s12902-015-0009-2
The relationship between N-terminal prosomatostatin, all-cause and cardiovascular mortality in patients with type 2 diabetes mellitus (ZODIAC-35)
Abstract
Background: The hormone somatostatin inhibits growth hormone release from the pituitary gland and is theoretically linked to diabetes and diabetes related complications. This study aimed to investigate the relationship between levels of the stable somatostatin precursor, N-terminal prosomatostatin (NT-proSST), with mortality in type 2 diabetes (T2DM) patients.
Methods: In 1,326 T2DM outpatients, participating in this ZODIAC prospective cohort study, Cox proportional hazards models were used to investigate the independent relationship between plasma NT-proSST concentrations with all-cause and cardiovascular mortality.
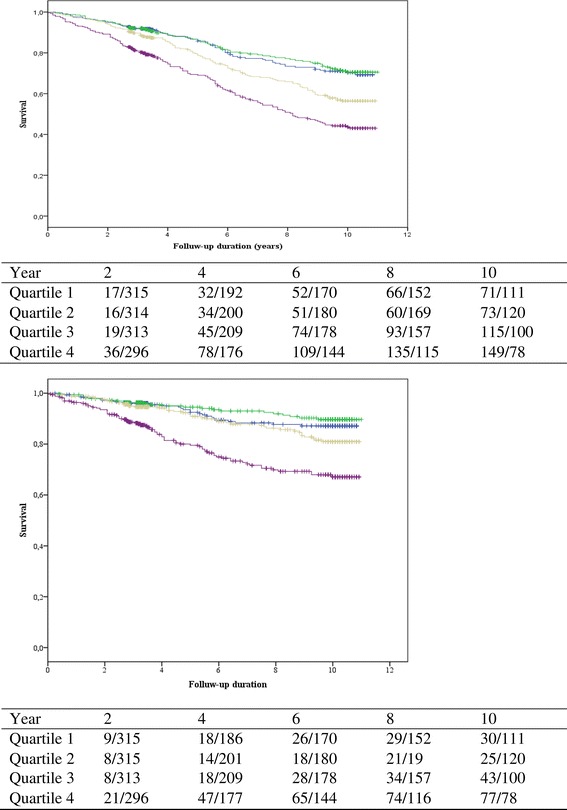
Results: Median concentration of NT-proSST was 592 [IQR 450-783] pmol/L. During follow-up for 6 [3-10] years, 413 (31%) patients died, of which 176 deaths (43%) were attributable to cardiovascular causes. The age and sex adjusted hazard ratios (HRs) for all-cause and cardiovascular mortality were 1.48 (95%CI 1.14 - 1.93) and 2.21 (95%CI 1.49 - 3.28). However, after further adjustment for cardiovascular risk factors there was no independent association of log NT-proSST with mortality, which was almost entirely attributable to adjustment for serum creatinine. There were no significant differences in Harrell's C statistics to predict mortality for the models with and without NT-proSST: both 0.79 (95%CI 0.77 - 0.82) and 0.81 (95%CI 0.77 - 0.84).
Conclusions: NT-proSST is unsuitable as a biomarker for cardiovascular and all-cause mortality in stable outpatients with T2DM.
Figures
Similar articles
-
N-Terminal Prosomatostatin as a Risk Marker for Cardiovascular Disease and Diabetes in a General Population.J Clin Endocrinol Metab. 2016 Sep;101(9):3437-44. doi: 10.1210/jc.2016-1736. Epub 2016 Jul 11. J Clin Endocrinol Metab. 2016. PMID: 27399347 Free PMC article. Clinical Trial.
-
Plasma N-terminal Prosomatostatin and Risk of Incident Cardiovascular Disease and All-Cause Mortality in a Prospective Observational Cohort: the PREVEND Study.Clin Chem. 2017 Jan;63(1):278-287. doi: 10.1373/clinchem.2016.259275. Epub 2016 Oct 25. Clin Chem. 2017. PMID: 28062624
-
Is the association of serum sodium with mortality in patients with type 2 diabetes explained by copeptin or NT-proBNP? (ZODIAC-46).Atherosclerosis. 2015 Sep;242(1):179-85. doi: 10.1016/j.atherosclerosis.2015.07.010. Epub 2015 Jul 8. Atherosclerosis. 2015. PMID: 26201002
-
Serum uric acid as a risk factor of all-cause mortality and cardiovascular events among type 2 diabetes population: Meta-analysis of correlational evidence.J Diabetes Complications. 2019 Oct;33(10):107409. doi: 10.1016/j.jdiacomp.2019.07.006. Epub 2019 Jul 25. J Diabetes Complications. 2019. PMID: 31439471
-
Hemoglobin glycation index in relationship to the risk of cardiovascular complication in patients with type 2 diabetes: A systematic review and meta-analysis.J Diabetes Complications. 2020 Oct;34(10):107673. doi: 10.1016/j.jdiacomp.2020.107673. Epub 2020 Jul 10. J Diabetes Complications. 2020. PMID: 32768332
Cited by
-
N-Terminal Prosomatostatin as a Risk Marker for Cardiovascular Disease and Diabetes in a General Population.J Clin Endocrinol Metab. 2016 Sep;101(9):3437-44. doi: 10.1210/jc.2016-1736. Epub 2016 Jul 11. J Clin Endocrinol Metab. 2016. PMID: 27399347 Free PMC article. Clinical Trial.
References
-
- Yamada T, Soll AH, Park J, Elashoff J. Autonomic regulation of somatostatin release: studies with primary cultures of canine fundic mucosal cells. Am J Physiol. 1984;247(5 Pt 1):G567–73. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
