

Mechanical ventilation modes for respiratory distress syndrome in infants: a systematic review and network meta-analysis
- PMID: 25881121
- PMCID: PMC4391657
- DOI: 10.1186/s13054-015-0843-7
Mechanical ventilation modes for respiratory distress syndrome in infants: a systematic review and network meta-analysis
Abstract
Introduction: The effects of different mechanical ventilation (MV) modes on mortality outcome in infants with respiratory distress syndrome (RDS) are not well known.
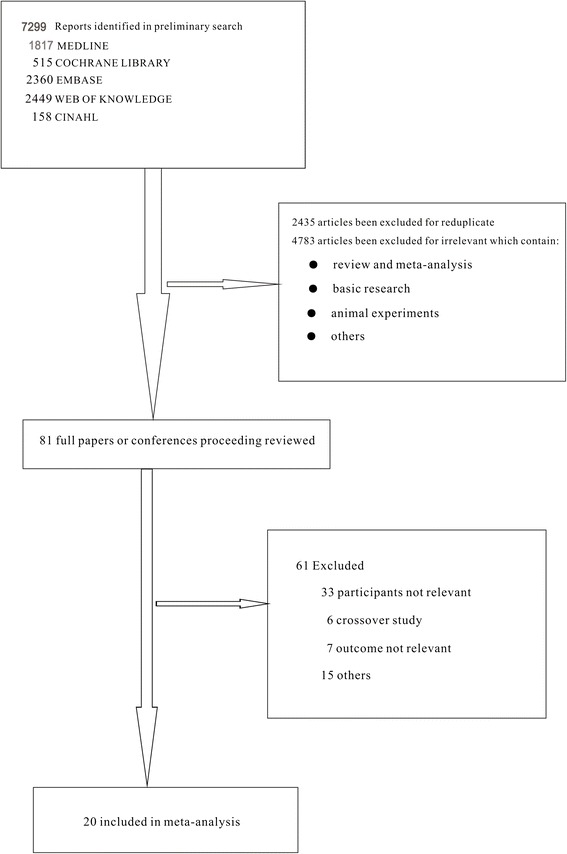
Methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library, EMBASE, MEDLINE, CINAHL, and Web of Science for studies published through April 2014 that assessed mortality in infants with RDS given different MV modes. We assessed studies for eligibility, extracted data, and subsequently pooled the data. A Bayesian fixed-effects model was used to combine direct comparisons with indirect evidence. We also performed sensitivity analyses and rankings of the competing treatment modes.
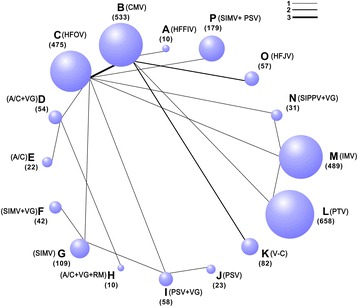
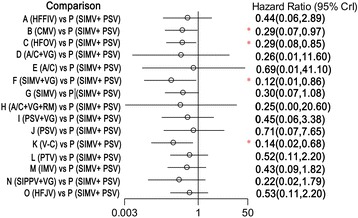
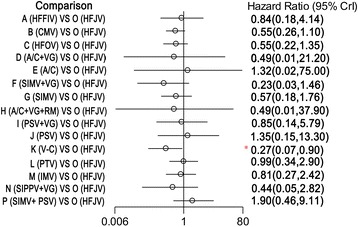
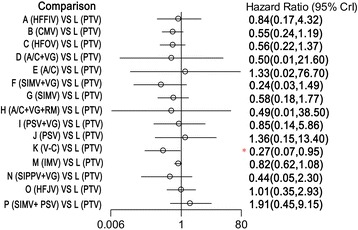
Results: In total, 20 randomized controlled trials were included for the network meta-analysis, which consisted of 2,832 patients who received one of 16 ventilation modes. Compared with synchronized intermittent mandatory ventilation (SIMV) + pressure support ventilation (PSV), time-cycled pressure-limited ventilation (TCPL) (hazard ratio (HR) 0.290; 95% confidence interval (CI) 0.071 to 0.972), high-frequency oscillatory ventilation (HFOV) (HR 0.294; 95% CI 0.080 to 0.852), SIMV + volume-guarantee (VG) (HR 0.122; 95% CI 0.014 to 0.858), and volume-controlled (V-C) (HR 0.139; 95% CI 0.024 to 0.677) ventilation modes are associated with lower mortality. The combined results of available ventilation modes were not significantly different in regard to the incidences of patent ductus arteriosus and intraventricular hemorrhage.
Conclusion: Compared with the SIMV + PSV ventilation mode, the TCPL, HFOV, SIMV + VG, and V-C ventilation modes are associated with lower mortality.
Figures
References
-
- Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European Association of Perinatal Medicine. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants–2013 update. Neonatology. 2013;103:353–68. doi: 10.1159/000349928. - DOI - PubMed
-
- Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European Association of Perinatal Medicine. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants - 2010 update.Neonatology. 2010;97:402–417. - PubMed
-
- Perelman RH, Farrell PM. Analysis of causes of neonatal death in the United States with specific emphasis on fatal hyaline membrane disease. Pediatrics. 1982;70:570–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
