

Optimal timing for elective egg freezing
- PMID: 25881876
- PMCID: PMC4457646
- DOI: 10.1016/j.fertnstert.2015.03.002
Optimal timing for elective egg freezing
Abstract
Objective: To estimate the optimal age to pursue elective oocyte cryopreservation.
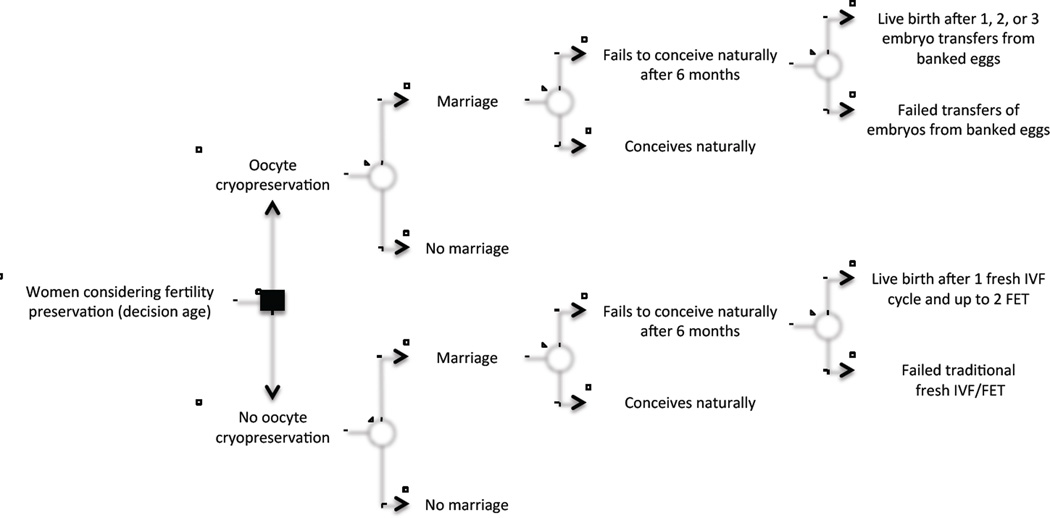
Design: A decision-tree model was constructed to determine the success and cost-effectiveness of oocyte preservation versus no action when considered at ages 25-40 years, assuming an attempt at procreation 3, 5, or 7 years after initial decision.
Setting: Not applicable.
Patient(s): Hypothetical patients 25-40 years old presenting to discuss elective oocyte cryopreservation.
Intervention(s): Decision to cryopreserve oocytes from age 25 years to age 40 years versus taking no action.
Main outcome and measure(s): Probability of live birth after initial decision whether or not to cryopreserve oocytes.
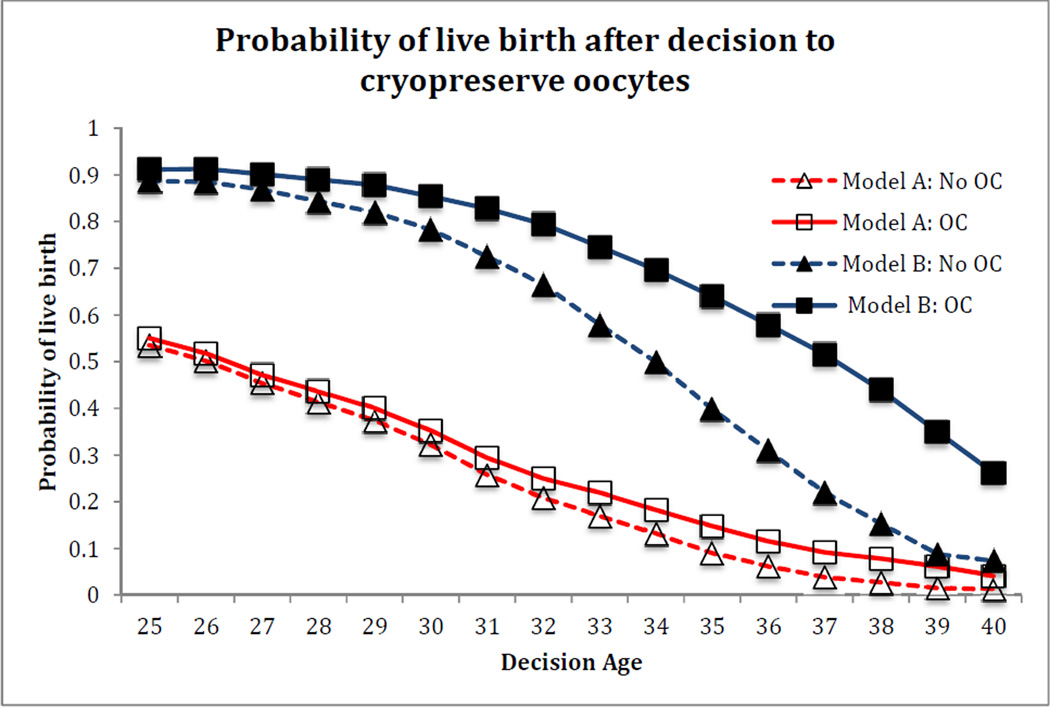
Result(s): Oocyte cryopreservation provided the greatest improvement in probability of live birth compared with no action (51.6% vs. 21.9%) when performed at age 37 years. The highest probability of live birth was seen when oocyte cryopreservation was performed at ages <34 years (>74%), although little benefit over no action was seen at ages 25-30 years (2.6%-7.1% increase). Oocyte cryopreservation was most cost-effective at age 37 years, at $28,759 per each additional live birth in the oocyte cryopreservation group. When the probability of marriage was included, oocyte cryopreservation resulted in little improvement in live birth rates.
Conclusion(s): Oocyte cryopreservation can be of great benefit to specific women and has the highest chance of success when performed at an earlier age. At age 37 years, oocyte cryopreservation has the largest benefit over no action and is most cost-effective.
Keywords: Elective oocyte cryopreservation; egg freezing; fertility preservation.
Copyright © 2015 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Martin JA, Hamilton BE, Ventura SJ. National vital statistics reports. 1. Vol. 62. Hyattsville, MD: National Center for Health Statistics; 2012. Births: final data for 2011. (DHHS publication no. 2014–1120). - PubMed
-
- Mathews TJ, Hamilton BE. NCHS data brief, no 21. Hyattsville, MD: National Center for Health Statistics; 2009. Delayed childbearing: More women are having their first child later in life. (DHHS publication no. (PHS) 2009–1209). - PubMed
-
- ESHRE Capri Workshop Group. Social determinants of human reproduction. Hum Reprod. 2001;16:1518–1526. - PubMed
-
- Kreider RM, Ellis R. Current population reports. Washington, DC: U.S. Census Bureau; 2011. Number, timing, and duration of marriages and divorces 2009; pp. 70–125.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
