

Nasal high flow clears anatomical dead space in upper airway models
- PMID: 25882385
- PMCID: PMC4482836
- DOI: 10.1152/japplphysiol.00934.2014
Nasal high flow clears anatomical dead space in upper airway models
Abstract
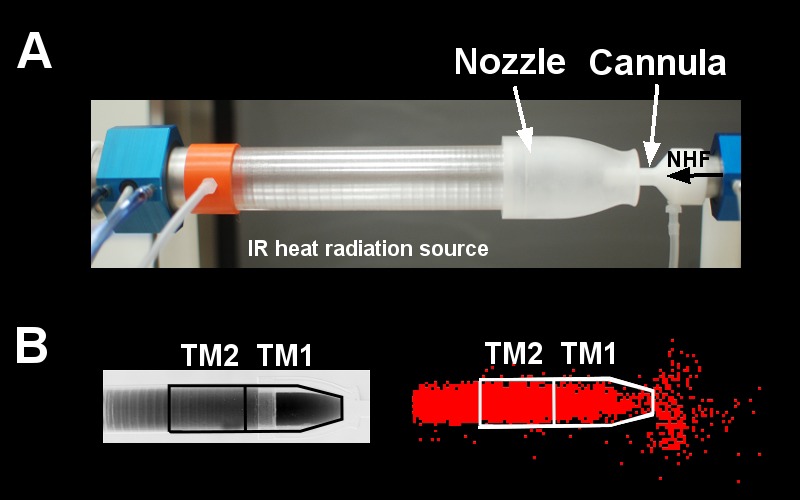
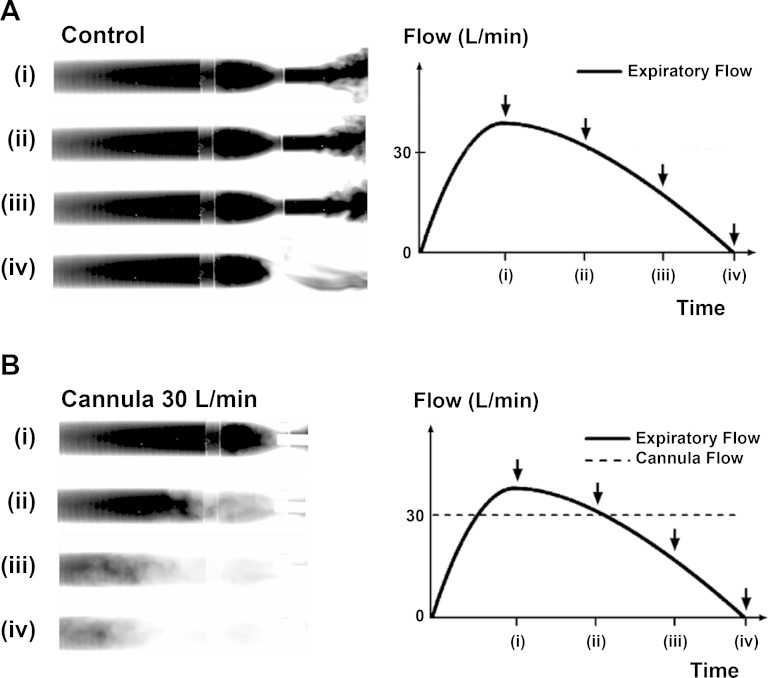
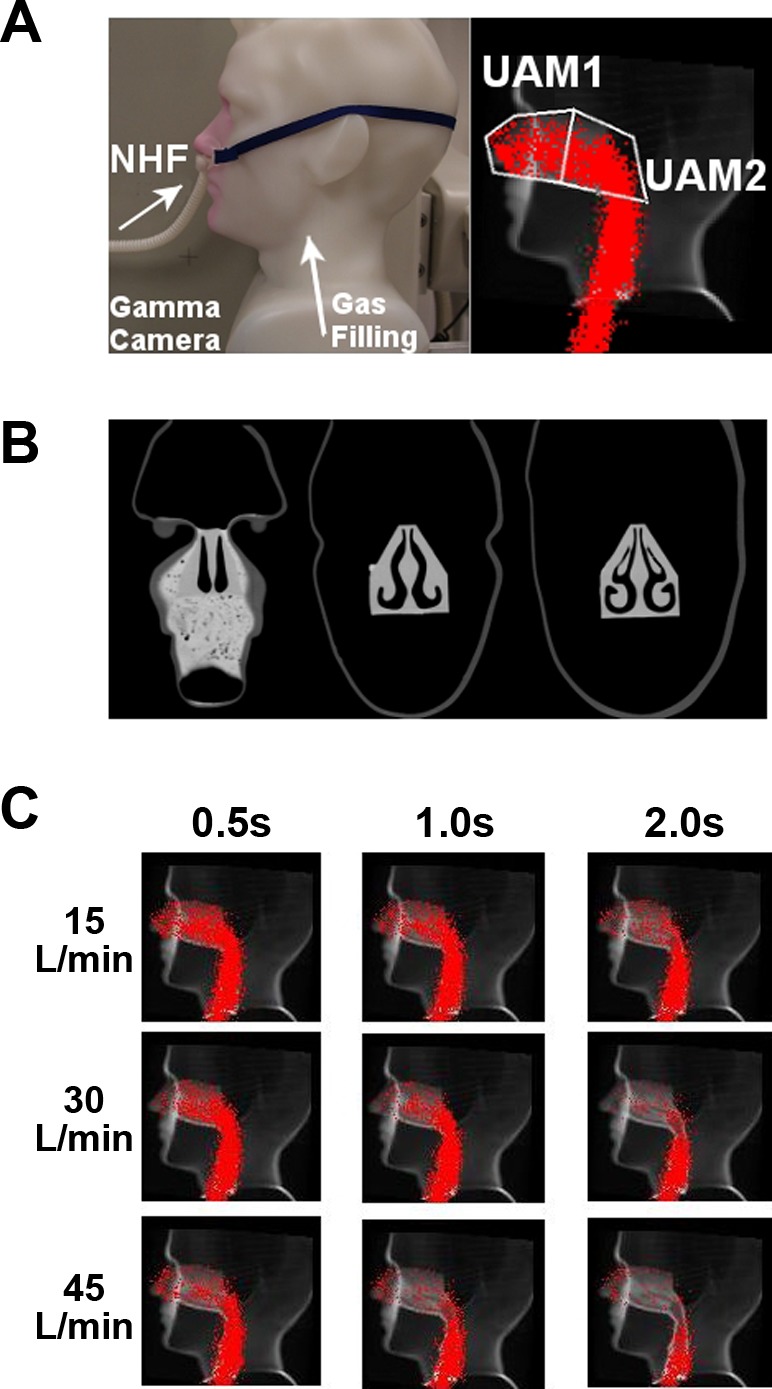
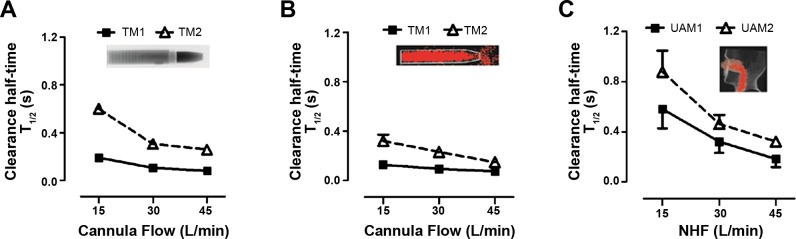
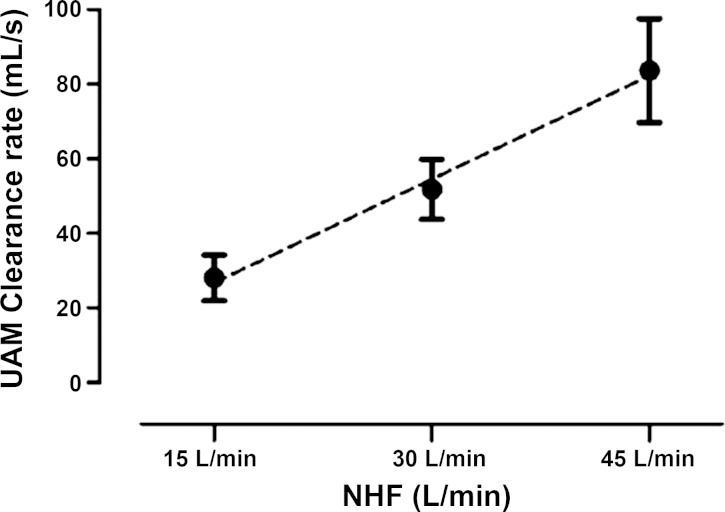
Recent studies showed that nasal high flow (NHF) with or without supplemental oxygen can assist ventilation of patients with chronic respiratory and sleep disorders. The hypothesis of this study was to test whether NHF can clear dead space in two different models of the upper nasal airways. The first was a simple tube model consisting of a nozzle to simulate the nasal valve area, connected to a cylindrical tube to simulate the nasal cavity. The second was a more complex anatomically representative upper airway model, constructed from segmented CT-scan images of a healthy volunteer. After filling the models with tracer gases, NHF was delivered at rates of 15, 30, and 45 l/min. The tracer gas clearance was determined using dynamic infrared CO2 spectroscopy and 81mKr-gas radioactive gamma camera imaging. There was a similar tracer-gas clearance characteristic in the tube model and the upper airway model: clearance half-times were below 1.0 s and decreased with increasing NHF rates. For both models, the anterior compartments demonstrated faster clearance levels (half-times < 0.5 s) and the posterior sections showed slower clearance (half-times < 1.0 s). Both imaging methods showed similar flow-dependent tracer-gas clearance in the models. For the anatomically based model, there was complete tracer-gas removal from the nasal cavities within 1.0 s. The level of clearance in the nasal cavities increased by 1.8 ml/s for every 1.0 l/min increase in the rate of NHF. The study has demonstrated the fast-occurring clearance of nasal cavities by NHF therapy, which is capable of reducing of dead space rebreathing.
Figures
References
-
- Ari A, Harwood R, Sheard M, Dailey P, Fink JB. In vitro comparison of heliox and oxygen in aerosol delivery using pediatric high flow nasal cannula. Pediatr Pulmonol 46: 795–801, 2011. - PubMed
-
- Bott J, Carroll MP, Conway JH, Keilty SEJ, Ward EM, Brown AM, Paul EA, Elliott MW, Godfrey RC, Wedzicha JA, Moxham J. Randomised controlled trial of nasal ventilation in acute ventilatory failure due to chronic obstructive airways disease. Lancet 341: 1555–1557, 1993. - PubMed
-
- Bräunlich J, Beyer D, Mai D, Hammerschmidt S, Seyfarth HJ, Wirtz H. Effects of nasal high flow on ventilation in volunteers, COPD and idiopathic pulmonary fibrosis patients. Respiration 85: 319–325, 2013. - PubMed
-
- Dhand R. Aerosol therapy in patients receiving noninvasive positive pressure ventilation. J Aerosol Med Pulm Drug Deliv 25: 63–78, 2011. - PubMed
-
- Dysart K, Miller TL, Wolfson MR, Shaffer TH. Research in high flow therapy: mechanisms of action. Respir Med 103: 1400–1405, 2009. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical