

Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs Health Care System
- PMID: 25882486
- PMCID: PMC4401870
- DOI: 10.1136/bmjopen-2015-007771
Multimorbidity and healthcare utilisation among high-cost patients in the US Veterans Affairs Health Care System
Abstract
Objectives: To investigate the relationship between multimorbidity and healthcare utilisation patterns among the highest cost patients in a large, integrated healthcare system.
Design: In this retrospective cross-sectional study of all patients in the U.S. Veterans Affairs (VA) Health Care System, we aggregated costs of individuals' outpatient and inpatient care, pharmacy services and VA-sponsored contract care received in 2010. We assessed chronic condition prevalence, multimorbidity as measured by comorbidity count, and multisystem multimorbidity (number of body systems affected by chronic conditions) among the 5% highest cost patients. Using multivariate regression, we examined the association between multimorbidity and healthcare utilisation and costs, adjusting for age, sex, race/ethnicity, marital status, homelessness and health insurance status.
Setting: USA VA Health Care System.
Participants: 5.2 million VA patients.
Measures: Annual total costs; absolute and share of costs generated through outpatient, inpatient, pharmacy and VA-sponsored contract care; number of visits to primary, specialty and mental healthcare; number of emergency department visits and hospitalisations.
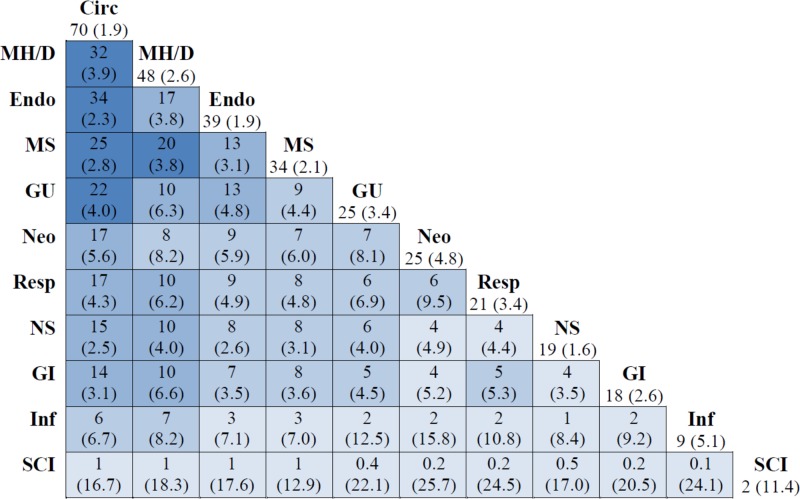
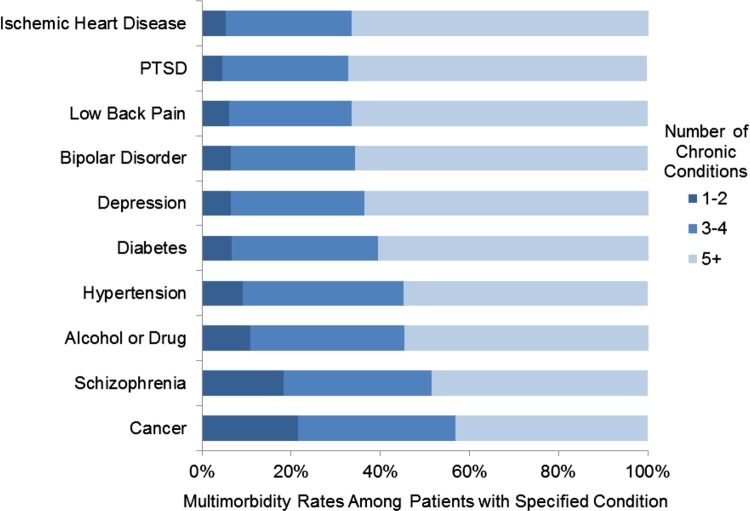
Results: The 5% highest cost patients (n=261,699) accounted for 47% of total VA costs. Approximately two-thirds of these patients had chronic conditions affecting ≥3 body systems. Patients with cancer and schizophrenia were less likely to have documented comorbid conditions than other high-cost patients. Multimorbidity was generally associated with greater outpatient and inpatient utilisation. However, increased multisystem multimorbidity was associated with a higher outpatient share of total costs (1.6 percentage points per affected body system, p<0.01) but a lower inpatient share of total costs (-0.6 percentage points per affected body system, p<0.01).
Conclusions: Multisystem multimorbidity is common among high-cost VA patients. While some patients might benefit from disease-specific programmes, for most patients with multimorbidity there is a need for interventions that coordinate and maximise efficiency of outpatient services across multiple conditions.
Keywords: GERIATRIC MEDICINE; HEALTH SERVICES ADMINISTRATION & MANAGEMENT; PRIMARY CARE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Cohen S, Uberoi N. Differentials in the concentration in the level of health expenditures across population subgroups in the U.S., 2010. Rockville, MD: Agency for Healthcare Research and Quality Statistical Brief #421, 2013. http://meps.ahrq.gov/mepsweb/data_files/publications/st421/stat421.shtml (accessed 22 Jan 15). - PubMed
-
- Sommers A, Cohen M. Medicaid's High Cost Enrollees: How Much Do They Drive Program Spending? Washington, DC: Kaiser Commission for Medicaid and the Uninsured, 2006.
-
- Garber AM, MaCurdy TE, McClellan MB. Persistence of Medicare expenditures among elderly beneficiaries. In: Garber AM, ed. Frontiers in Health Policy Research. Vol 1 Cambridge, MA: MIT, 1998:153–80.
-
- Cohen S, Yu W. AHRQ Statistical Brief #354: The concentration and persistence in the level of health expenditures over time: Estimates for the US population, 2008–2009 2012. http://meps.ahrq.gov/mepsweb/data_files/publications/st354/stat354.pdf (accessed 28 Nov 2012).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical