

The association between colonization with carbapenemase-producing enterobacteriaceae and overall ICU mortality: an observational cohort study
- PMID: 25882764
- PMCID: PMC4431676
- DOI: 10.1097/CCM.0000000000001028
The association between colonization with carbapenemase-producing enterobacteriaceae and overall ICU mortality: an observational cohort study
Abstract
Objectives: Infections caused by carbapenemase-producing Enterobacteriaceae are increasing worldwide, especially in ICUs, and have been associated with high mortality rates. However, unequivocally demonstrating causality of such infections to death is difficult in critically ill patients because of potential confounding and competing events. Here, we quantified the effects of carbapenemase-producing Enterobacteriaceae carriage on patient outcome in two Greek ICUs with carbapenemase-producing Enterobacteriaceae endemicity.
Design: Observational cohort study.
Setting: Two ICUs with carbapenemase-producing Enterobacteriaceae endemicity.
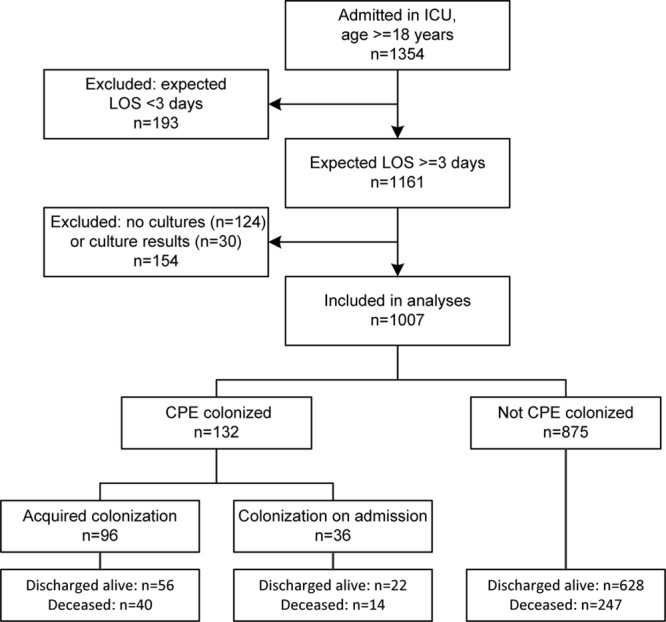
Patients: Patients admitted to the ICU with an expected length of ICU stay of at least 3 days were included.
Interventions: None.
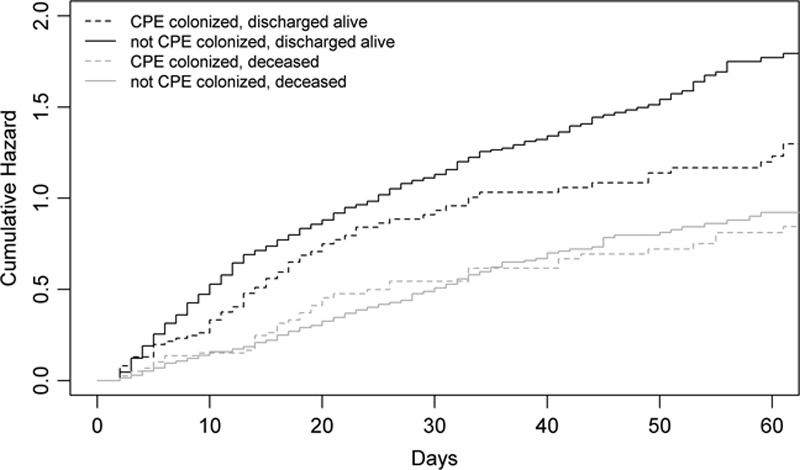
Measurements and main results: Carbapenemase-producing Enterobacteriaceae colonization was established through screening in perineum swabs obtained at admission and twice weekly and inoculated on chromogenic plates. Detection of carbapenemases was performed phenotypically, with confirmation by polymerase chain reaction. Risk factors for ICU mortality were evaluated using cause-specific hazard ratios and subdistribution hazard ratios, with carbapenemase-producing Enterobacteriaceae colonization as time-varying covariate. One thousand seven patients were included, 36 (3.6%) were colonized at admission, and 96 (9.5%) acquired carbapenemase-producing Enterobacteriaceae colonization during ICU stay, and 301 (29.9%) died in ICU. Of 132 carbapenemase-producing Enterobacteriaceae isolates, 125 (94.7%) were Klebsiella pneumoniae and 74 harbored K. pneumoniae carbapenemase (56.1%), 54 metallo-β-lactamase (40.9%), and four both (3.0%). Carbapenemase-producing Enterobacteriaceae colonization was associated with a statistically significant increase of the subdistribution hazard ratio for ICU mortality (subdistribution hazard ratio=1.79; 95% CI, 1.31-2.43), not explained by an increased daily hazard of dying (cause-specific hazard ratio for death=1.02; 95% CI, 0.74-1.41), but by an increased length of stay (cause-specific hazard ratio for discharge alive=0.73; 95% CI, 0.51-0.94). Other risk factors in the subdistribution hazard model were Acute Physiology and Chronic Health Evaluation II score (subdistribution hazard ratio=1.13; 95% CI, 1.11-1.15), female gender (subdistribution hazard ratio=1.29; 95% CI, 1.02-1.62), presence of solid tumor (subdistribution hazard ratio=1.54; 95% CI, 1.15-2.06), hematopoietic malignancy (subdistribution hazard ratio=1.61; 95% CI, 1.04-2.51), and immunodeficiency (subdistribution hazard ratio=1.59; 95% CI, 1.11-2.27).
Conclusions: Patients colonized with carbapenemase-producing Enterobacteriaceae have on average a 1.79 times higher hazard of dying in ICU than noncolonized patients, primarily because of an increased length of stay.
Conflict of interest statement
Dr. Dautzenberg’s institution received grant support from the European Commission (EC) under the Life Science Health Priority of the 6th Framework Program (Mastering hOSpital Antimicrobial Resistance in Europe [MOSAR] network contract LSHP-CT-2007-037941). Dr. Gniadkowski consulted for European Centre for Disease Prevention and Control and European Society of Clinical Microbiology and Infectious Diseases (Dr. Gniadkwoski is a member of the Scientific Advisory Board of the EuSCAPE Surveillance project. He is a member of the Subcommittee for Scientific Affairs of the European Society of Clinical Microbiology and Infectious Disesease [travel costs]), provided expert testimony for the National Research Centre, Poland (Dr. Gniadkwoski is a member of the Expert Board reviewing grant applications for the National Research Centre), lectured for Liofilchem (support for travel and honorarium), received support for travel from bioMerieux, and received support for article research from the EC grant by MOSAR. His institution received grant support from the EC (institution participated in the EC project MOSAR within which this study was performed), National Research Center Poland, and Liofilchem (Dr. Gniadkowski’s team ran/is running a number of research grants from different entities). Dr. Giamarellou consulted for Astellas, Novartis, and Pfizer and lectured for Pfizer and Novartis. Dr. Petrikkos’ institution received grant support from the National and Kapodistrian University of Athens. Dr. Skiada received support for travel from the MOSAR study. Dr. Skiada and her institution received grant support from the MOSAR study. Dr. Brun-Buisson’s institution received grant support from the EC (MOSAR Integrated Project). Dr. Bonten’s institution received grant support from the EU 7th Framework Program. Dr. Derde is employed by UMC Utrecht. Her institution received grant support from the EC under the Life Science Health Priority of the 6th Framework Program (MOSAR network contract LSHP-CT-2007-037941). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Hazard Ratios and Hazardous Carbapenemase-Producing Enterobacteriaceae.Crit Care Med. 2015 Nov;43(11):e536-7. doi: 10.1097/CCM.0000000000001233. Crit Care Med. 2015. PMID: 26468729 No abstract available.
-
The authors reply.Crit Care Med. 2015 Nov;43(11):e537-8. doi: 10.1097/CCM.0000000000001291. Crit Care Med. 2015. PMID: 26468730 No abstract available.
References
-
- Gupta N, Limbago BM, Patel JB, et al. Carbapenem-resistant Enterobacteriaceae: Epidemiology and prevention. Clin Infect Dis. 2011;53:60–67. - PubMed
-
- Walsh TR. Emerging carbapenemases: A global perspective. Int J Antimicrob Agents. 2010;36(Suppl 3):S8–S14. - PubMed
-
- Nordmann P, Poirel L. The difficult-to-control spread of carbapenemase producers among Enterobacteriaceae worldwide. Clin Microbiol Infect. 2014;20:821–830. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
