

Biodistribution and radiation dosimetry for a probe targeting prostate-specific membrane antigen for imaging and therapy
- PMID: 25883128
- PMCID: PMC5003538
- DOI: 10.2967/jnumed.115.156133
Biodistribution and radiation dosimetry for a probe targeting prostate-specific membrane antigen for imaging and therapy
Abstract
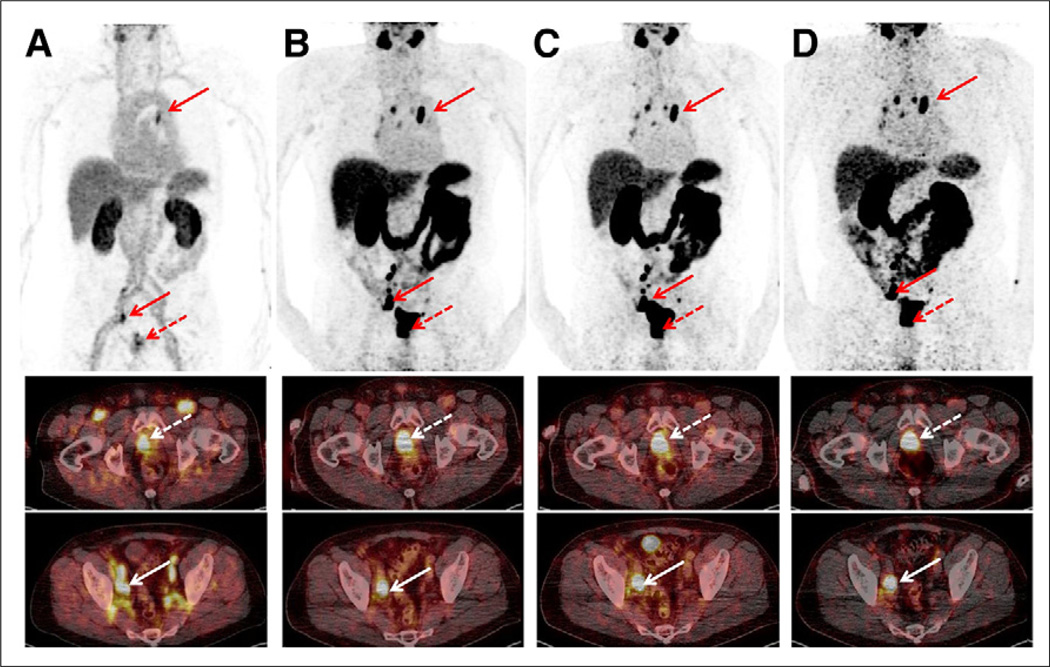
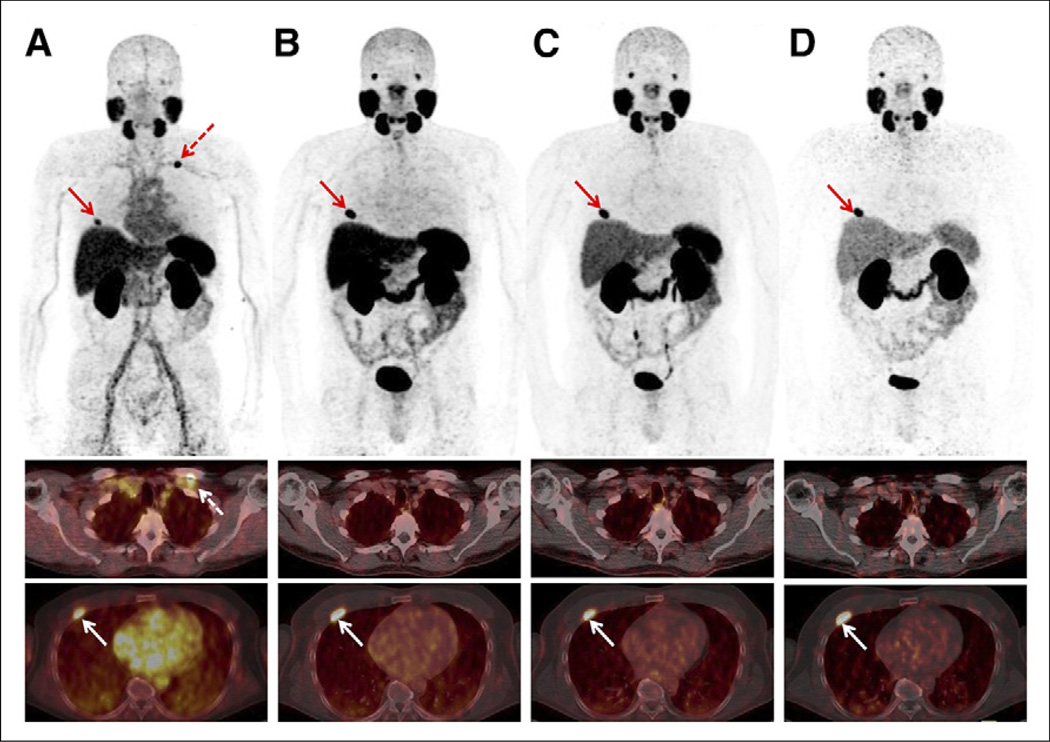
Prostate-specific membrane antigen (PSMA) is a promising target for diagnosis and treatment of prostate cancer. EuK-Subkff-(68)Ga-DOTAGA ((68)Ga-PSMA Imaging & Therapy [PSMA I&T]) is a recently introduced PET tracer for imaging PSMA expression in vivo. Whole-body distribution and radiation dosimetry of this new probe were evaluated.
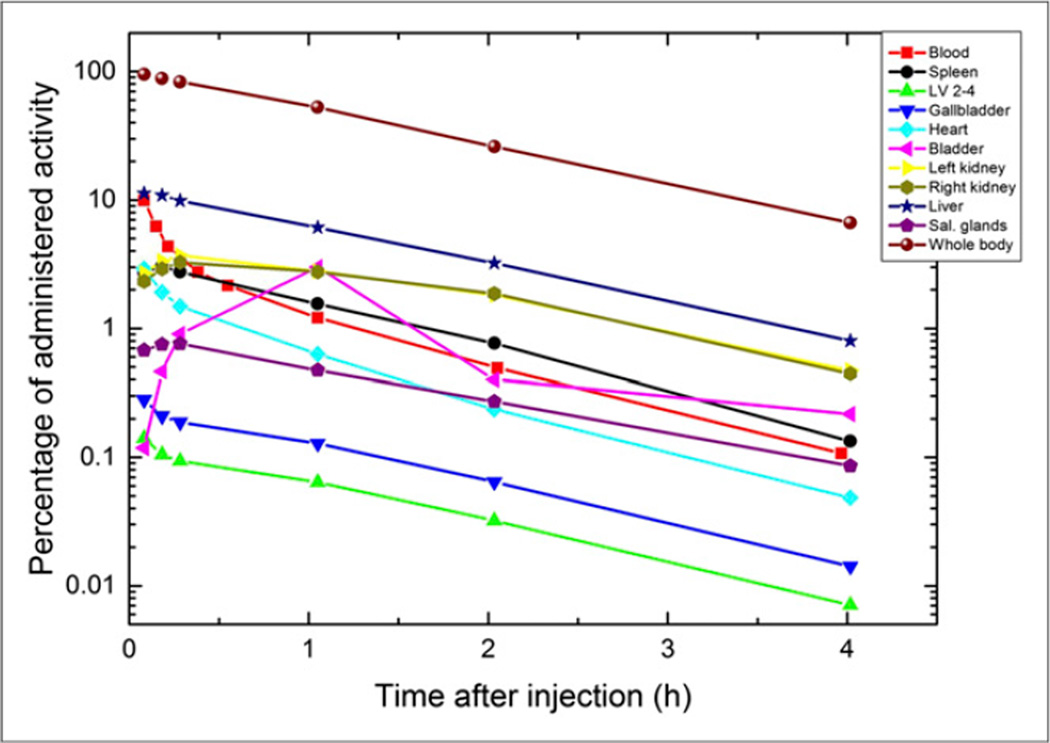
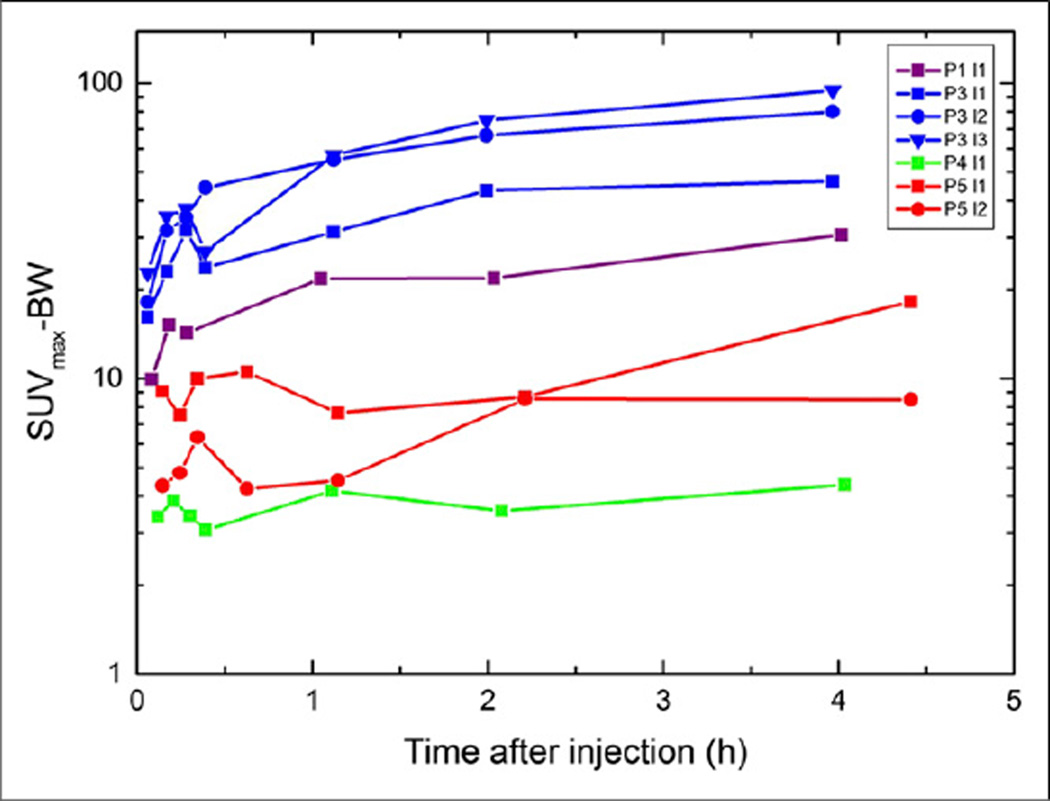
Methods: Five patients with a history of prostate cancer were injected intravenously with 91-148 MBq of (68)Ga-PSMA I&T (mean ± SD, 128 ± 23 MBq). After an initial series of rapid whole-body scans, 3 static whole-body scans were acquired at 1, 2, and 4 h after tracer injection. Time-dependent changes of the injected activity per organ were determined. Mean organ-absorbed doses and effective doses were calculated using OLINDA/EXM.
Results: Injection of 150 MBq of (68)Ga-PSMA I&T resulted in an effective dose of 3.0 mSv. The kidneys were the critical organ (33 mGy), followed by the urinary bladder wall and spleen (10 mGy each), salivary glands (9 mGy each), and liver (7 mGy).
Conclusion: (68)Ga-PSMA I&T exhibits a favorable dosimetry, delivering organ doses that are comparable to (kidneys) or lower than those delivered by (18)F-FDG.
Keywords: 68Ga; PET; PSMA; dosimetry; prostate cancer.
© 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Beer AJ, Eiber M, Souvatzoglou M, Schwaiger M, Krause BJ. Radionuclide and hybrid imaging of recurrent prostate cancer. Lancet Oncol. 2011;12:181–191. - PubMed
-
- Schöder H, Herrmann K, Gonen M, et al. 2-[18F]fluoro-2-deoxyglucose positron emission tomography for the detection of disease in patients with prostate-specific antigen relapse after radical prostatectomy. Clin Cancer Res. 2005;11:4761–4769. - PubMed
-
- Shiiba M, Ishihara K, Kimura G, et al. Evaluation of primary prostate cancer using 11C-methionine-PET/CT and 18F-FDG-PET/CT. Ann Nucl Med. 2012;26:138–145. - PubMed
-
- Nanni C, Schiavina R, Boschi S, et al. Comparison of 18F-FACBC and 11C-choline PET/CT in patients with radically treated prostate cancer and biochemical relapse: preliminary results. Eur J Nucl Med Mol Imaging. 2013;40(suppl 1):S11–S17. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous