

Randomized phase 2 trial of NP001-a novel immune regulator: Safety and early efficacy in ALS
- PMID: 25884010
- PMCID: PMC4396529
- DOI: 10.1212/NXI.0000000000000100
Randomized phase 2 trial of NP001-a novel immune regulator: Safety and early efficacy in ALS
Abstract
Objective: To assess the safety, tolerability, and preliminary efficacy of NP001, a novel immune regulator of inflammatory monocytes/macrophages, for slowing progression of amyotrophic lateral sclerosis (ALS).
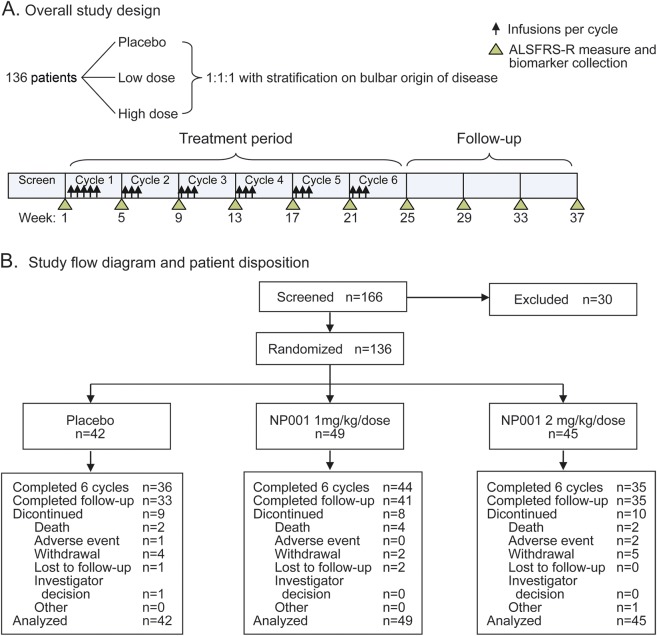
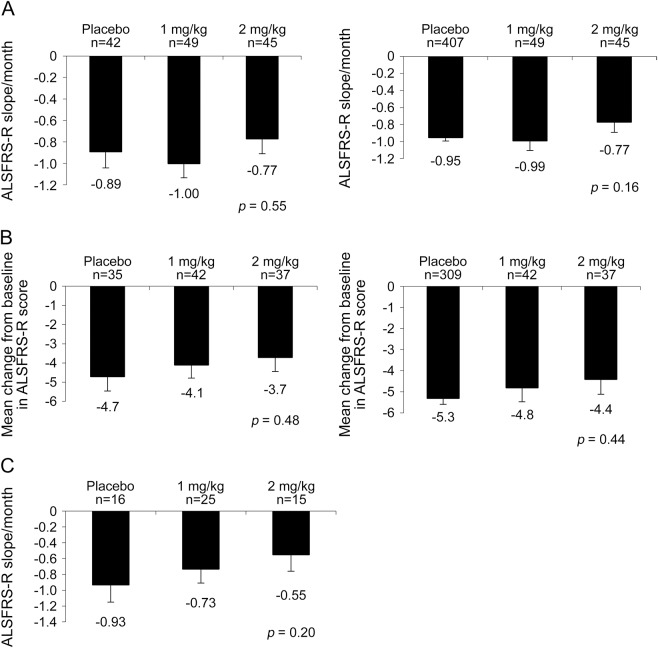
Methods: This was a phase 2 randomized, double-blind, placebo-controlled trial of NP001 in 136 patients with ALS of <3 years' duration and forced vital capacity ≥70%. Participants received NP001 2 mg/kg, NP001 1 mg/kg, or placebo for 6 months. Safety, tolerability, and inflammatory biomarkers were assessed throughout the study. Preliminary efficacy was evaluated using the ALS Functional Rating Scale-Revised (ALSFRS-R) slope and change from baseline, with and without matched historical placebo controls, after 6 months of treatment. A post hoc analysis of the percentage of patients ("responders") whose ALSFRS-R did not change from baseline was also conducted.
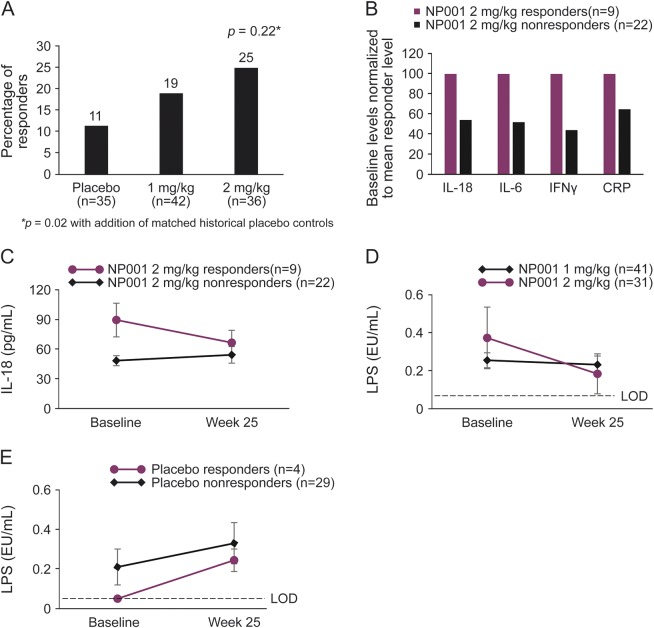
Results: NP001 was generally safe and well-tolerated, except for infusion site pain and dizziness. No significant slowing of decline in the primary or secondary measures was observed. However, slowing of progression was observed in the high-dose group in patients with greater inflammation (wide range C-reactive protein). Moreover, NP001 may have dose dependently halted symptom progression in a subset of patients. More than 2 times as many patients on high-dose NP001 (25%) did not progress during 6 months of treatment compared with those on placebo (11%). Most "responders" had an elevated biomarker of inflammation, interleukin-18, and were positive for lipopolysaccharide at baseline, which decreased after treatment with NP001.
Conclusion: The arresting of progression of ALS symptoms by NP001 in a subset of patients with marked neuroinflammation, as observed here, will represent a novel therapeutic approach for patients with ALS, if confirmed.
Classification of evidence: This study provides Class I evidence that for patients with ALS, NP001 is safe and did not significantly slow progression of the disease (difference in slope of the ALSFRS-R/month 0.12 favoring NP001, p = 0.55). The study lacks the precision to exclude an important effect of NP001.
Figures
References
-
- Boillée S, Vande Velde C, Cleveland DW. ALS: a disease of motor neurons and their nonneuronal neighbors. Neuron 2006;52:39–59. - PubMed
-
- Henkel JS, Beers DR, Zhao W, Appel SH. Microglia in ALS: the good, the bad, and the resting. J Neuroimmune Pharmacol 2009;4:389–398. - PubMed
-
- Turner MR, Kiernan MC, Leigh PN, Talbot K. Biomarkers in amyotrophic lateral sclerosis. Lancet Neurol 2009;8:94–109. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous