

A patient develops transient unique cerebral and cerebellar lesions after unruptured aneurysm coiling
- PMID: 25884179
- PMCID: PMC4387739
- DOI: 10.1186/s12883-015-0303-7
A patient develops transient unique cerebral and cerebellar lesions after unruptured aneurysm coiling
Abstract
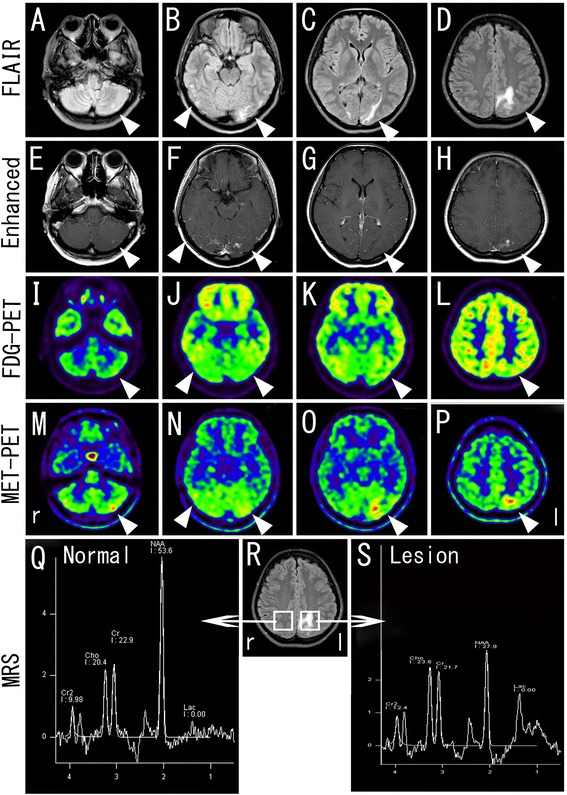
Background: We describe a case of a very unusual complication following a coiling procedure in which the patient developed transient unique cerebral and cerebellar lesions. Lesions were examined not only by magnetic resonance imaging (MRI) but also by positron emission tomography-computed tomography (PET-CT) and proton magnetic resonance spectroscopy ((1)H-MRS).
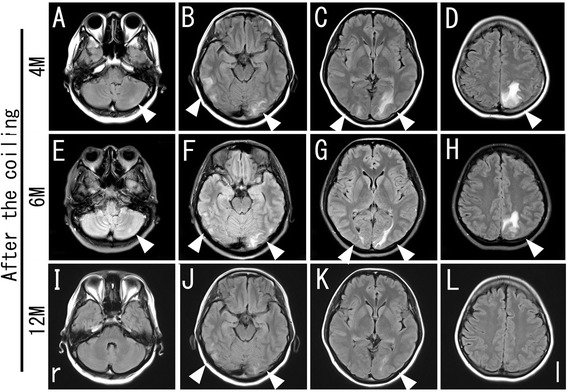
Case presentation: A 33-year-old woman presented an incidental 3.7 × 3.3-mm unruptured cerebral aneurysm (CAn) in her basilar artery, which was successfully coiled with balloon assistance. A follow-up brain MRI at 1 and 2 months showed a gradual increase in several white matter hyperintense lesions in the left cerebellar, bilateral occipitotemporal and left parietoccipital lobe during fluid-attenuated inversion recovery (FLAIR). These were the only lesions associated with perfused CAn. However, the patient did not show any additional symptoms such as visual disturbance throughout the entire course. (11)C-methionine-PET (MET-PET) showed an obvious increase in methionine uptake in the lesion corresponding to enhanced areas with gadolinium-enhanced MRI. MRS showed a decrease in the N-acetylaspartate/creatine (NAA/cr) ratio and a slight elevation of the choline/creatine (cho/cr) ratio and a lactate peak in the lesion. A follow-up MRI at 6 and 12 months showed a gradual decrease in the initial hyperintense lesions in FLAIR without any treatment.
Conclusion: We present a case of an unusual complication after a coiling procedure. Although it is difficult to identify this etiology without a pathological examination, it is importance to increase awareness of such a potential complication arising from coiling procedures, because interventional procedures have become the first choice of treatment for cerebrovascular diseases in many countries.
Figures

References
-
- Rahal JP, Malek AM. Clip occlusion versus coil embolization for the treatment of cerebral aneurysms. J Neurosurg Sci. 2012;56(3):175–190. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
