

Trends in paediatric bloodstream infections at a South African referral hospital
- PMID: 25884449
- PMCID: PMC4396163
- DOI: 10.1186/s12887-015-0354-3
Trends in paediatric bloodstream infections at a South African referral hospital
Abstract
Background: The epidemiology of paediatric bloodstream infection (BSI) in Sub-Saharan Africa is poorly documented with limited data on hospital-acquired sepsis, impact of HIV infection, BSI trends and antimicrobial resistance.
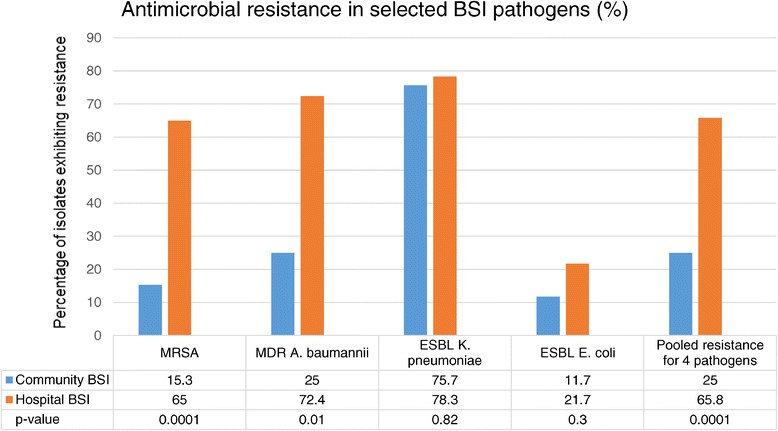
Methods: We retrospectively reviewed paediatric BSI (0-14 years) at Tygerberg Children's Hospital between 1 January 2008 and 31 December 2013 (excluding neonatal wards). Laboratory and hospital data were used to determine BSI rates, blood culture contamination, pathogen profile, patient demographics, antimicrobial resistance and factors associated with mortality. Fluconazole resistant Candida species, methicillin-resistant Staphylococcus aureus (MRSA), multi-drug resistant Acinetobacter baumannii and extended-spectrum beta-lactamase (ESBL) producing Enterobacteriaceae were classified as antimicrobial resistant pathogens.
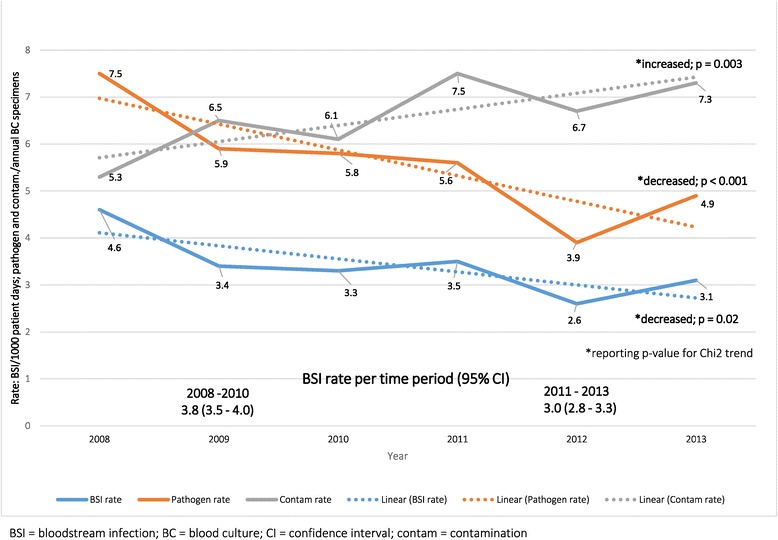
Results: Of 17001 blood cultures over 6 years, 935 cultures isolated 979 pathogens (5.5% yield; 95% CI 5.3-5.7%). Contamination rates were high (6.6%, 95% CI 6.4-6.8%), increasing over time (p = 0.003). Discrete BSI episodes were identified (n = 864) with median patient age of 7.5 months, male predominance (57%) and 13% HIV prevalence. BSI rates declined significantly over time (4.6-3.1, overall rate 3.5 per 1000 patient days; 95% CI 3.3-3.7; Chi square for trend p = 0.02). Gram negative pathogens predominated (60% vs 33% Gram positives and 7% fungal); Klebsiella pneumoniae (154; 17%), Staphylococcus aureus (131; 14%) and Escherichia coli (97; 11%) were most prevalent. Crude BSI mortality was 20% (176/864); HIV infection, fungal, Gram negative and hospital-acquired sepsis were significantly associated with mortality on multivariate analysis. Hospital-acquired BSI was common (404/864; 47%). Overall antimicrobial resistance rates were high (70% in hospital vs 25% in community-acquired infections; p < 0.0001); hospital-acquired infection, infancy, HIV-infection and Gram negative sepsis were associated with resistance. S. pneumoniae BSI declined significantly over time (58/465 [12.5%] to 33/399 [8.3%]; p =0.04).
Conclusion: Although BSI rates declined over time, children with BSI had high mortality and pathogens exhibited substantial antimicrobial resistance in both community and hospital-acquired infections. Blood culture sampling technique and local options for empiric antimicrobial therapy require re-evaluation.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
