

Laparoscopic versus open appendectomy in patients with suspected appendicitis: a systematic review of meta-analyses of randomised controlled trials
- PMID: 25884671
- PMCID: PMC4399217
- DOI: 10.1186/s12876-015-0277-3
Laparoscopic versus open appendectomy in patients with suspected appendicitis: a systematic review of meta-analyses of randomised controlled trials
Abstract
Background: Several systematic reviews (SRs) of randomised controlled trials (RCTs) comparing laparoscopic versus open appendectomy have been published, but there has been no overview of SRs of these two interventions. This overview (review of review) aims to summarise the results of such SRs in order to provide the most up to date evidence, and to highlight discordant results.
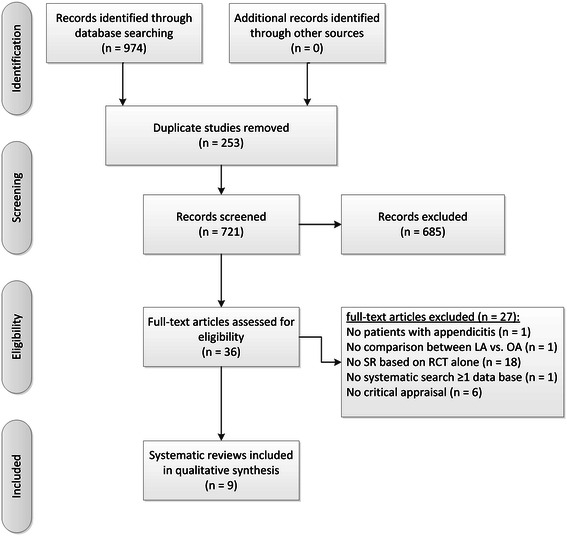
Methods: Medline, Embase, Cinahl, the Cochrane Database of Systematic Reviews and the Database of Abstracts of Reviews of Effects were searched for SRs published up to August 2014. Study selection and quality assessment using the AMSTAR tool were carried out independently by two reviewers. We used standardised forms to extract data that were analysed descriptively.
Results: Nine SRs met the inclusion criteria. All were of moderate to high quality. The number of randomized controlled trials (RCTs) they included ranged from eight to 67. The duration of surgery pooled by eight reviews was 7.6 to 18.3 minutes shorter using the open approach. Pain scores on the first postoperative day were lower after laparoscopic appendectomy in two out of three reviews. The risk of abdominal abscesses was higher for laparoscopic surgery in half of six meta-analyses. The occurrence of wound infections pooled by all reviews was lower after laparoscopic appendectomy. One review showed no difference in mortality. The laparoscopic approach shortened hospital stay from 0.16 to 1.13 days in seven out of eight meta-analyses, though the strength of the evidence was affected by strong heterogeneity.
Conclusion: Laparoscopic and open appendectomy are both safe and effective procedures for the treatment of acute appendicitis. This overview shows discordant results with respect to the magnitude of the effect but not to the direction of the effect. The evidence from this overview may prove useful for the development of clinical guidelines and protocols.
References
-
- Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–25. - PubMed
-
- Becker LA, Oxman AD. Chapter 22: Overviews of reviews. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
