

Cancers of unknown primary origin (CUP) are characterized by chromosomal instability (CIN) compared to metastasis of know origin
- PMID: 25885340
- PMCID: PMC4404593
- DOI: 10.1186/s12885-015-1128-x
Cancers of unknown primary origin (CUP) are characterized by chromosomal instability (CIN) compared to metastasis of know origin
Abstract
Background: Cancers of unknown primary (CUPs) constitute ~5% of all cancers. The tumors have an aggressive biological and clinical behavior. The aim of the present study has been to uncover whether CUPs exhibit distinct molecular features compared to metastases of known origin.
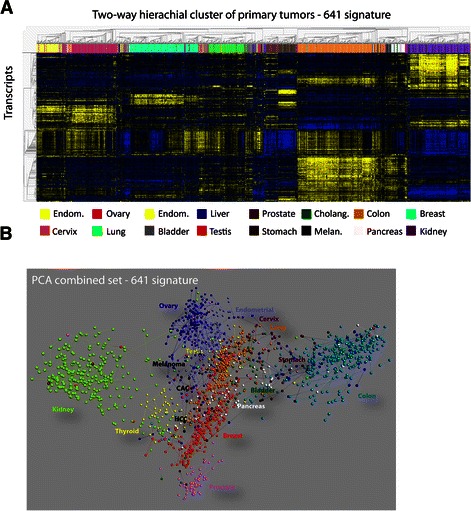
Methods: Employing genome wide transcriptome analysis, Linear Discriminant Analysis (LDA) and Quadratic Discriminant Analysis (QDA), we defined the putative origins of a large series of CUP and how closely related a particular CUP was to corresponding metastases of known origin. LDA predictions were subsequently used to define a universal CUP core set of differentially expressed genes, that by means of gene set enrichment analysis was exploited to depict molecular pathways characterizing CUP.
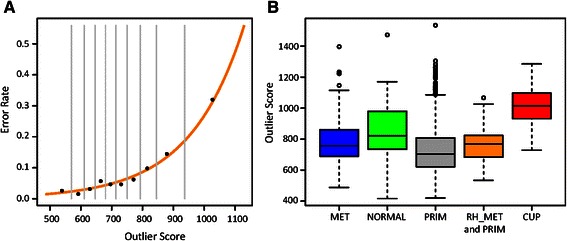
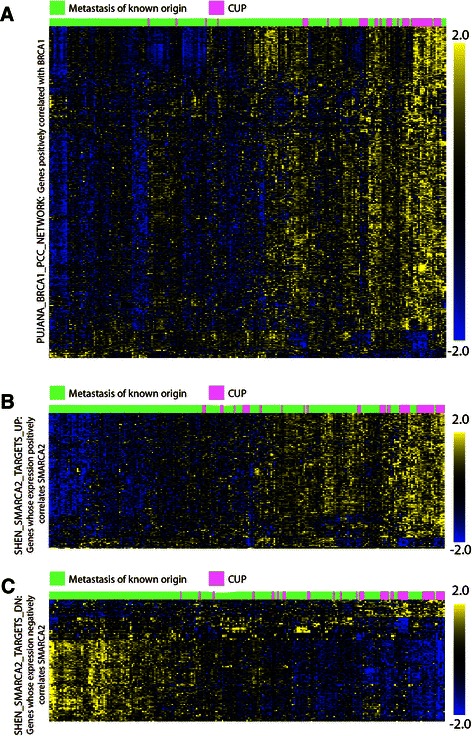
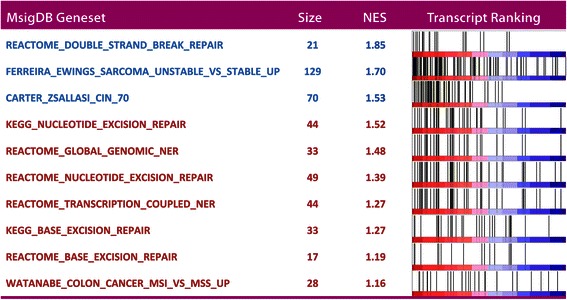
Results: The analyses show that CUPs are distinct from metastases of known origin. CUPs exhibit inconsistent expression of conventional cancer biomarkers and QDA derived outlier scores show that CUPs are more distantly related to their primary tumor class than corresponding metastases of known origin. Gene set enrichment analysis showed that CUPs display increased expression of genes involved in DNA damage repair and mRNA signatures of chromosome instability (CIN), indicating that CUPs are chromosome unstable compared to metastases of known origin.
Conclusions: CIN may account for the uncommon clinical presentation, chemoresistance and poor outcome in patients with CUP and warrant selective diagnostic strategies and treatment.
Figures


References
-
- Daugaard G, Møller A, Petersen B. Carcinoma of Unknown Primary. In: Cavalli HH F, Kaye S, Amritage J, Pickard M, editors. Textbook of Medical Oncology. 4. 2009. pp. 313–22.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
