

Systemic lupus erythematous and malignancy risk: a meta-analysis
- PMID: 25885411
- PMCID: PMC4401738
- DOI: 10.1371/journal.pone.0122964
Systemic lupus erythematous and malignancy risk: a meta-analysis
Abstract
Background: Pilot studies have estimated cancer incidence in patients with systemic lupus erythematous (SLE). However, the results have been inconclusive. To ascertain the correlation between SLE and malignancy more comprehensively and precisely, we conducted a meta-analysis.
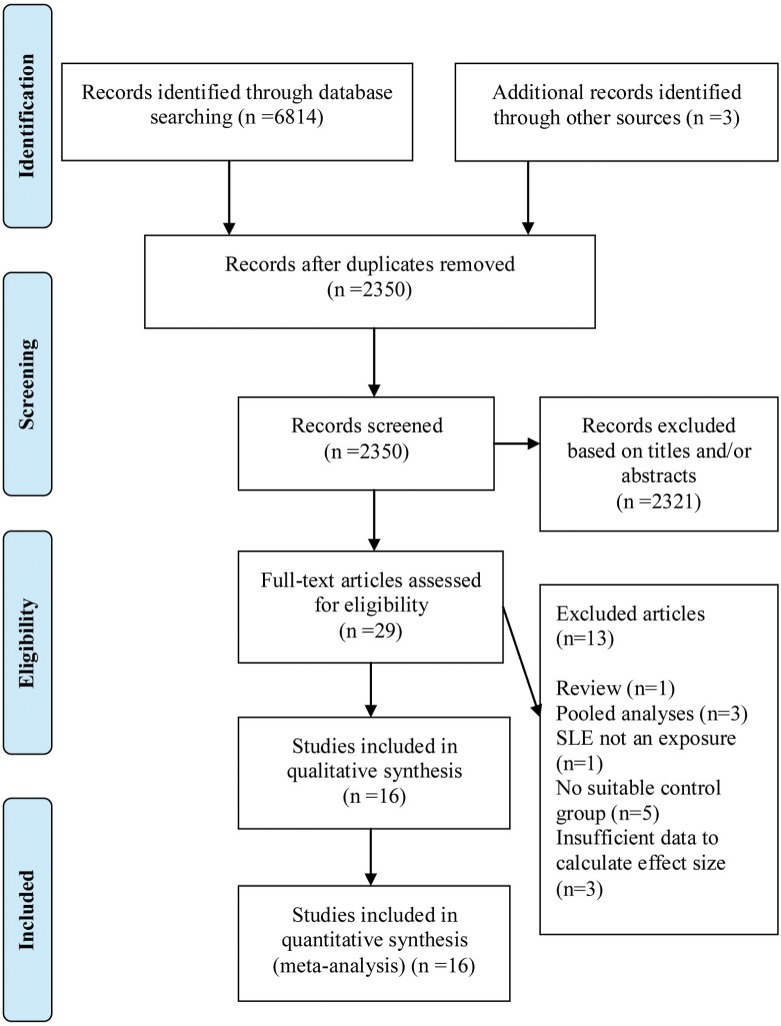
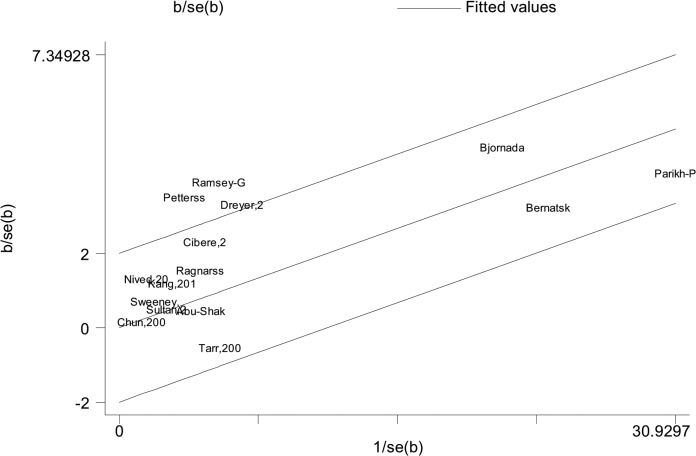
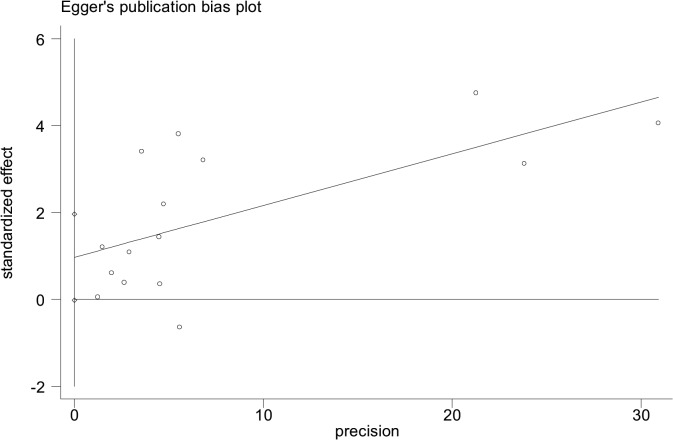
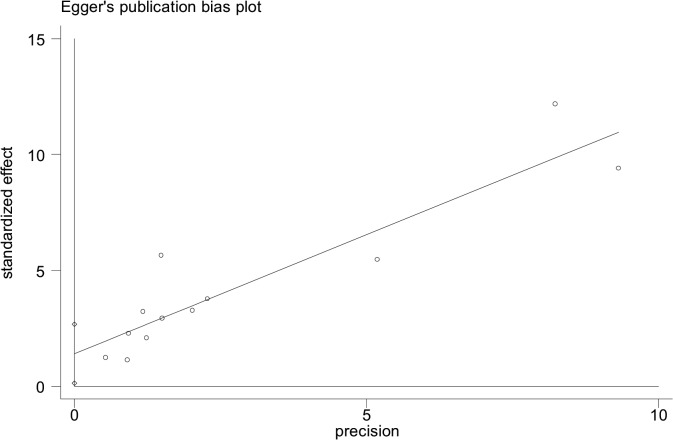
Methods: PubMed, the Cochrane Library and Embase databases through June 2014, were searched to identify observational studies evaluating the association between SLE and malignancy. The outcomes from these studies were measured as relative risks (RRs). A random or fixed effects model was chosen to calculate the pooled RR according to heterogeneity test. Between-study heterogeneity was assessed by estimating I2 index. Publication bias was assessed by Egger's test.
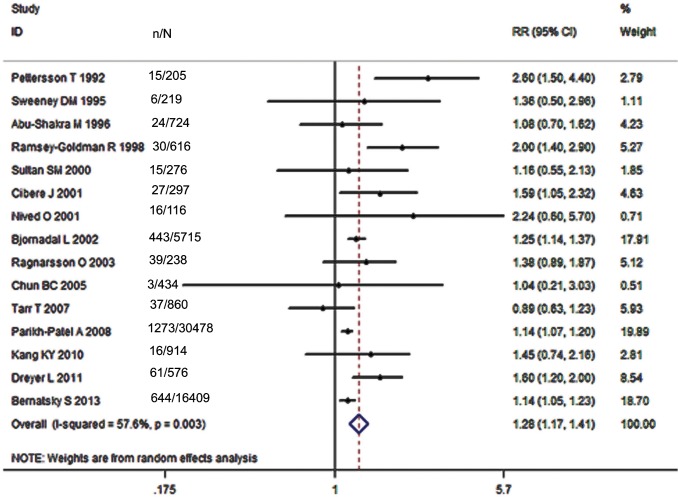
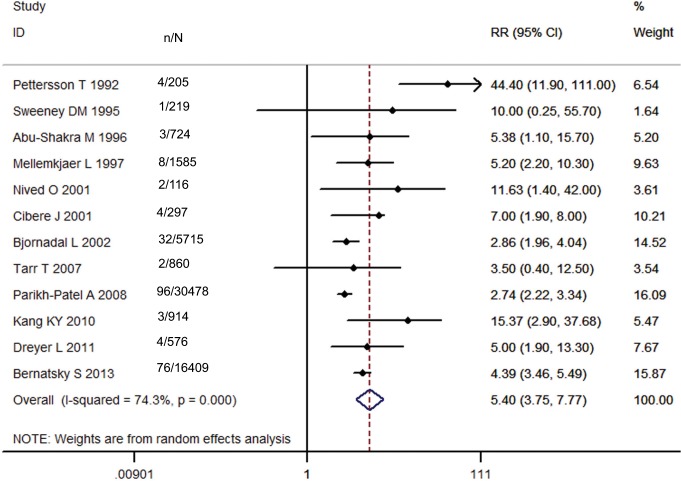
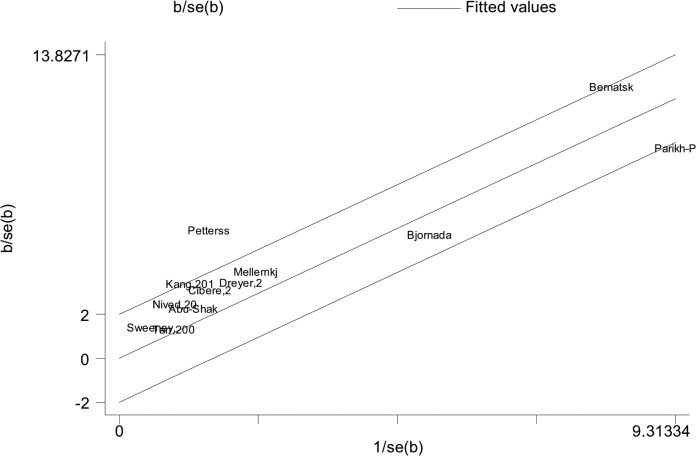
Results: A total of 16 papers, including 59,662 SLE patients, were suitable for the meta-analysis. Of these papers, 15 reported RRs for overall malignancy, 12 for non-Hodgkin lymphoma (NHL) and lung cancer, 7 for bladder cancer, 6 for Hodgkin lymphoma (HL) and leukemia, 5 for skin melanoma, and liver and thyroid cancers, 4 for multiple myeloma (MM), and esophageal and vaginal/vulvar cancers and 3 for laryngeal and non-melanoma skin cancers. The pooled RRs were 1.28 (95% CI, 1.17-1.41) for overall cancer, 5.40 (95% CI, 3.75-7.77) for NHL, 3.26(95% CI, 2.17-4.88) for HL, 2.01(95% CI, 1.61-2.52) for leukemia, 1.45(95% CI, 1.04-2.03) for MM, 4.19(95% CI, 1.98-8.87) for laryngeal cancer, 1.59 (95% CI, 1.44-1.76) for lung cancer, 1.86(95% CI, 1.21-2.88) for esophageal cancer, 3.21(95% CI, 1.70-6.05) for liver cancer, 3.67(95% CI, 2.80-4.81) for vaginal/vulvar cancer, 2.11(95% CI, 1.12-3.99) for bladder cancer, 1.51(95% CI, 1.12-2.03) for non-melanoma skin cancer, 1.78(95% CI, 1.35-2.33) for thyroid cancer, and 0.65(95% CI, 0.50-0.85) for skin melanoma. Only the meta-analyses of overall malignancy, NHL, and liver and bladder cancers produced substantial heterogeneity (I2, 57.6% vs 74.3% vs 67.7% vs 82.3%). No apparent publication bias was detected except for NHL studies.
Conclusions: Our data support an association between SLE and malignancy, not only demonstrating an increased risk for NHL, HL, leukemia, and some non-hematologic malignancies, including laryngeal, lung, liver, vaginal/vulvar, and thyroid malignancies, but also a reduced risk for skin melanoma. Although an increased risk of MM, and esophageal, bladder and non-melanoma skin cancers was identified from the accumulated data in these studies, this observation requires confirmation.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
