

Calcineurin inhibitors differentially alter the circadian rhythm of T-cell functionality in transplant recipients
- PMID: 25885792
- PMCID: PMC4329209
- DOI: 10.1186/s12967-015-0420-5
Calcineurin inhibitors differentially alter the circadian rhythm of T-cell functionality in transplant recipients
Abstract
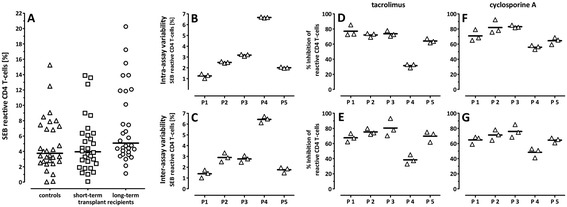
Background: Graft survival in transplant recipients depends on pharmacokinetics and on individual susceptibility towards immunosuppressive drugs. Nevertheless, pharmacodynamic changes in T-cell functionality in response to drugs and in relation to pharmacokinetics are poorly characterized. We therefore investigated the immunosuppressive effect of calcineurin inhibitors and steroids on general T-cell functionality after polyclonal stimulation of whole blood samples.
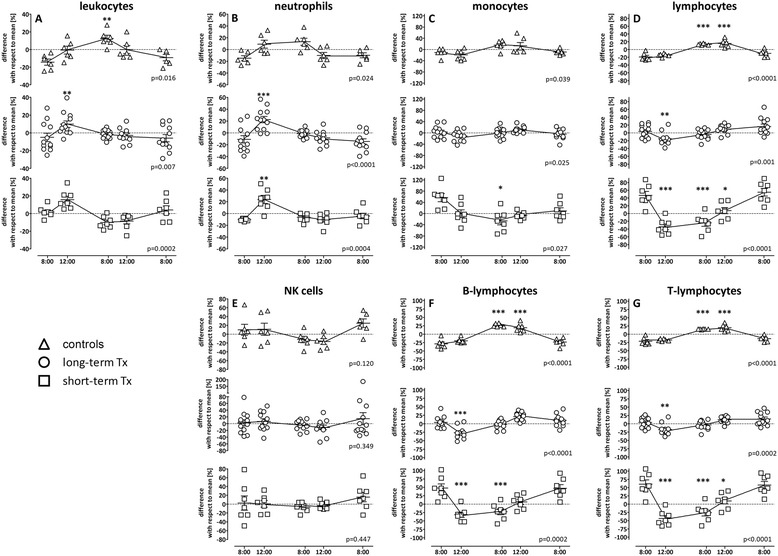
Methods: General T-cell functionality in the absence or presence of immunosuppressive drugs was determined in vitro directly from whole blood based on cytokine induction after stimulation with the polyclonal stimulus Staphylococcus aureus enterotoxin B. In addition, diurnal changes in leukocyte and lymphocyte subsets, and on T-cell function after intake of immunosuppressive drugs were analyzed in 19 patients during one day and compared to respective kinetics in six immunocompetent controls. Statistical analysis was performed using non-parametric and parametric tests.
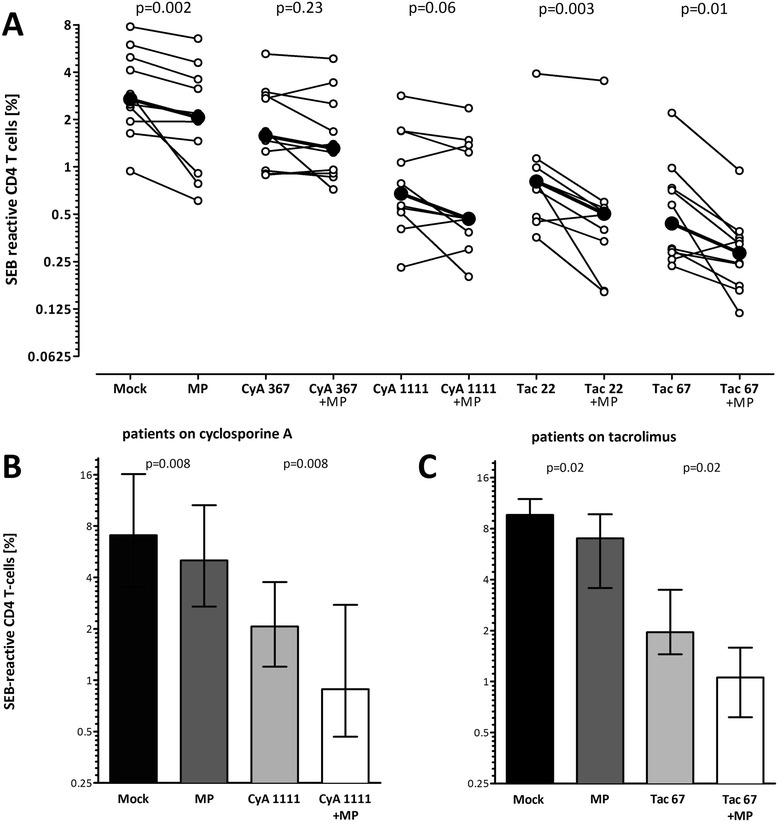
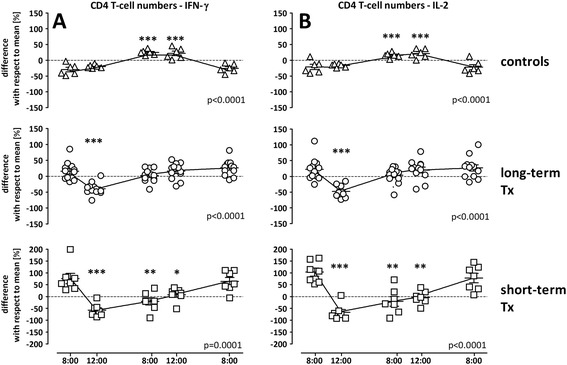
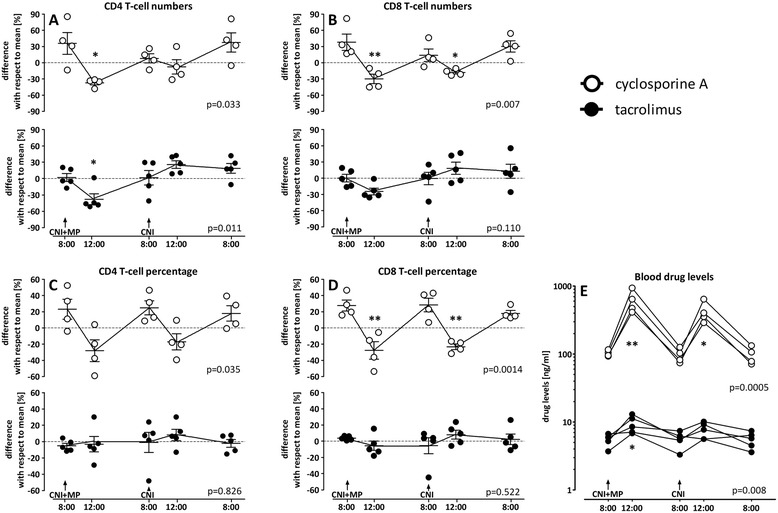
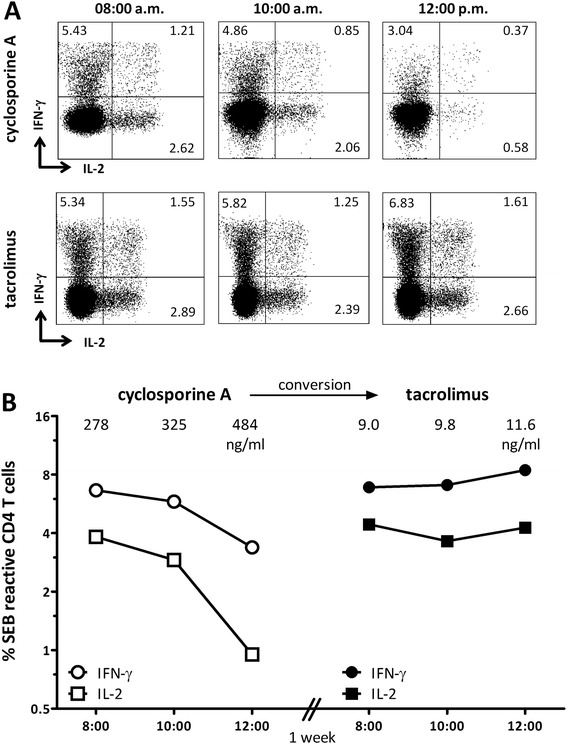
Results: Susceptibility towards calcineurin inhibitors showed interindividual differences. When combined with steroids, tacrolimus led to more pronounced increase in the inhibitory activity as compared to cyclosporine A. While circadian alterations in leukocyte subpopulations and T-cell function in controls were related to endogenous cortisol levels, T-cell functionality in transplant recipients decreased after intake of the morning medication, which was more pronounced in patients with higher drug-dosages. Interestingly, calcineurin inhibitors differentially affected circadian rhythm of T-cell function, as patients on cyclosporine A showed a biphasic decrease in T-cell reactivity after drug-intake in the morning and evening, whereas T-cell reactivity in patients on tacrolimus remained rather stable.
Conclusions: The whole blood assay allows assessment of the inhibitory activity of immunosuppressive drugs in clinically relevant concentrations. Circadian alterations in T-cell function are determined by dose and type of immunosuppressive drugs and show distinct differences between cyclosporine A and tacrolimus. In future these findings may have practical implications to estimate the net immunosuppressive effect of a given drug-regimen that daily acts in an individual patient, and may contribute to individualize immunosuppression.
Figures
Similar articles
-
Immune monitoring with a lymphocyte adenosine triphosphate assay in kidney transplant recipients treated with a calcineurin inhibitor.Exp Clin Transplant. 2014 Jun;12(3):195-9. Exp Clin Transplant. 2014. PMID: 24907718
-
Quantitative analysis of regulatory T cells in kidney graft recipients: a relationship with calcineurin inhibitor level.Transpl Immunol. 2009 May;21(1):43-9. doi: 10.1016/j.trim.2009.02.002. Epub 2009 Feb 20. Transpl Immunol. 2009. PMID: 19233271
-
Impaired erythropoietin production in liver transplant recipients: the role of calcineurin inhibitors.Liver Transpl. 2006 Nov;12(11):1649-54. doi: 10.1002/lt.20898. Liver Transpl. 2006. PMID: 17058250
-
Therapeutic monitoring of calcineurin inhibitors for the nephrologist.Clin J Am Soc Nephrol. 2007 Mar;2(2):374-84. doi: 10.2215/CJN.03791106. Epub 2007 Feb 14. Clin J Am Soc Nephrol. 2007. PMID: 17699437 Review.
-
Cyclosporine and tacrolimus for the treatment of rheumatoid arthritis.Curr Opin Rheumatol. 2007 May;19(3):238-45. doi: 10.1097/BOR.0b013e328099af80. Curr Opin Rheumatol. 2007. PMID: 17414949 Review.
Cited by
-
Convergence of Several Biorhythms in Immunosuppressive Therapy for Liver Transplantation: Commentary on Ushijima et al.Clin Pharmacol Ther. 2025 Aug;118(2):304-307. doi: 10.1002/cpt.3723. Epub 2025 May 25. Clin Pharmacol Ther. 2025. PMID: 40413759 No abstract available.
-
A Polyclonal Immune Function Assay Allows Dose-Dependent Characterization of Immunosuppressive Drug Effects but Has Limited Clinical Utility for Predicting Infection on an Individual Basis.Front Immunol. 2020 May 15;11:916. doi: 10.3389/fimmu.2020.00916. eCollection 2020. Front Immunol. 2020. PMID: 32499781 Free PMC article.
-
Tolerogenic Dendritic Cells on Transplantation: Immunotherapy Based on Second Signal Blockage.J Immunol Res. 2015;2015:856707. doi: 10.1155/2015/856707. Epub 2015 Oct 12. J Immunol Res. 2015. PMID: 26543876 Free PMC article. Review.
-
VZV-specific T-cell levels in patients with rheumatic diseases are reduced and differentially influenced by antirheumatic drugs.Arthritis Res Ther. 2018 Nov 9;20(1):252. doi: 10.1186/s13075-018-1742-5. Arthritis Res Ther. 2018. PMID: 30413189 Free PMC article.
-
Quantitative phosphoproteomics to unravel the cellular response to chemical stressors with different modes of action.Arch Toxicol. 2020 May;94(5):1655-1671. doi: 10.1007/s00204-020-02712-7. Epub 2020 Mar 18. Arch Toxicol. 2020. PMID: 32189037 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
