

Cost-effectiveness of active monitoring versus antidepressants for major depression in primary health care: a 12-month non-randomized controlled trial (INFAP study)
- PMID: 25885818
- PMCID: PMC4394418
- DOI: 10.1186/s12888-015-0448-3
Cost-effectiveness of active monitoring versus antidepressants for major depression in primary health care: a 12-month non-randomized controlled trial (INFAP study)
Abstract
Background: Clinical practice guidelines for the treatment of major depressive disorder (MDD) recommend antidepressants for patients with moderate-severe depression and active monitoring for patients with mild-moderate symptoms. The feasibility and efficiency of active monitoring has not been proven conclusively. The aim of this study is to evaluate the cost-effectiveness of active monitoring in comparison to antidepressants for primary care patients with mild-moderate MDD.
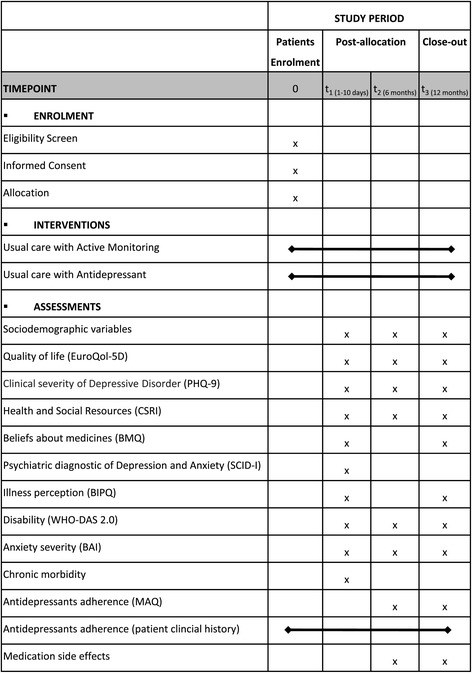
Methods/design: This is a 12-month follow-up multicenter observational prospective controlled trial. Patients are enrolled in 12 primary care centers in Barcelona (Spain). Eligible patients are adults (≥18 years-old) with a new episode of MDD that sign a written consent to participate. This is a naturalistic study in which general practitioners (GPs) use their professional judgment to allocate patients into active monitoring or antidepressants groups. GPs treat the patients following their clinical criteria. At baseline, GPs complete a questionnaire (sociodemographic/job characteristics, training, attitude towards depression, interest on mental health and participation in communication groups). Patients' measurements take place at baseline and after six and 12 months. Main outcome measures include severity of depression (PHQ-9), health-related quality of life (EuroQol-5D) and use of healthcare and social care services (Client Service Receipt Inventory). Secondary outcomes include diagnosis of MDD according to DSM-IV diagnostic criteria (SCID-I), disability (WHO-DAS), anxiety (BAI), comorbidities, medication side-effects and beliefs about medicines (BMQ). The analysis will be done according to the intention to treat analysis. Missing data will be imputed using multiple imputation by chained equations. To minimize the bias resulting from the lack of randomization, a propensity score will be used. Incremental effects and costs between groups will be modelled in each of the imputed databases using multivariate generalized linear models and then combined as per Rubin's rules. Propensity scores will be used to adjust the models. Incremental cost-effectiveness ratios will be calculated by dividing the difference in costs between groups by the difference in effects. To deal with the uncertainty, resampling techniques with bootstrapping will be used and cost-effectiveness planes and cost-effectiveness acceptability curves will be constructed. A series of sensitivity analyses will be performed.
Discussion: Given the high burden and costs generated by depressive disorder, it is important that general practitioners treat major depression efficiently. Recent evidence has suggested that antidepressants have low benefits for patients with mild to moderate major depression. For such cases of depression, active monitoring exists as a treatment option, but it is not without difficulties for implementation and its effectiveness and efficiency have not been demonstrated conclusively. The results of the study will provide information on which is the most efficient approach to treat patients with mild to moderate major depression in primary care.
Trial registration: ClinicalTrials.gov: NCT02245373.
Figures
References
-
- Golberg D, Huxley P. Common Mental Disorders: a Biosocial Model. London: Tavistock/Routledge; 1992.
-
- Serrano-Blanco A, Palao DJ, Luciano JV, Pinto-Meza A, Luján L, Fernández A, et al. Prevalence of mental disorders in primary care: Results from the diagnosis and treatment of mental disorders in primary care study (DASMAP) Soc Psychiatry Psychiatr Epidemiol. 2010;45:201–10. doi: 10.1007/s00127-009-0056-y. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
