

Copeptin levels are associated with organ dysfunction and death in the intensive care unit after out-of-hospital cardiac arrest
- PMID: 25886856
- PMCID: PMC4415235
- DOI: 10.1186/s13054-015-0831-y
Copeptin levels are associated with organ dysfunction and death in the intensive care unit after out-of-hospital cardiac arrest
Abstract
Introduction: We studied associations of the stress hormones copeptin and cortisol with outcome and organ dysfunction after out-of-hospital cardiac arrest (OHCA).
Methods: Plasma was obtained after consent from next of kin in the FINNRESUSCI study conducted in 21 Finnish intensive care units (ICUs) between 2010 and 2011. We measured plasma copeptin (pmol/L) and free cortisol (nmol/L) on ICU admission (245 patients) and at 48 hours (additional 33 patients). Organ dysfunction was categorised with 24-hour Sequential Organ Failure Assessment (SOFA) scores. Twelve-month neurological outcome (available in 276 patients) was classified with cerebral performance categories (CPC) and dichotomised into good (CPC 1 or 2) or poor (CPC 3 to 5). Data are presented as medians and interquartile ranges (IQRs). A Mann-Whitney U test, multiple linear and logistic regression tests with odds ratios (ORs) 95% confidence intervals (CIs) and beta (B) values, repeated measure analysis of variance, and receiver operating characteristic curves with area under the curve (AUC) were performed.
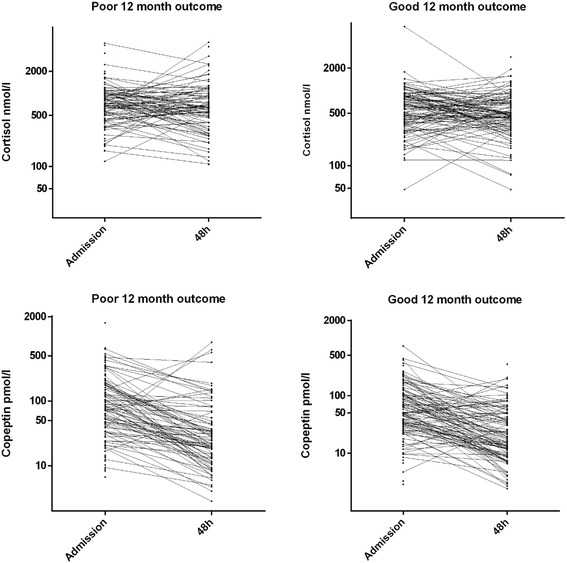
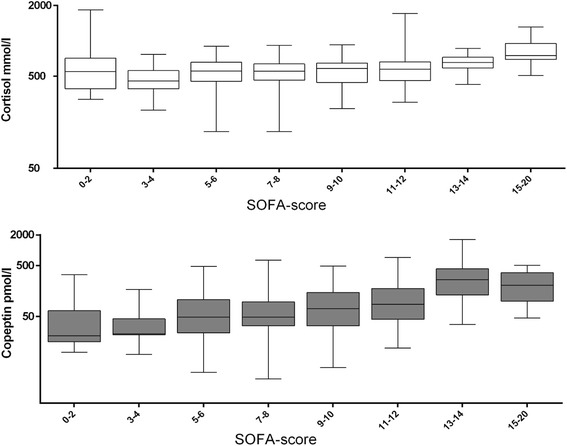
Results: Patients with a poor 12-month outcome had higher levels of admission copeptin (89, IQR 41 to 193 versus 51, IQR 29 to 111 pmol/L, P = 0.0014) and cortisol (728, IQR 522 to 1,017 versus 576, IQR 355 to 850 nmol/L, P = 0.0013). Copeptin levels fell between admission and 48 hours (P <0.001), independently of outcome (P = 0.847). Cortisol levels did not change between admission and 48 hours (P = 0.313), independently of outcome (P = 0.221). The AUC for predicting long-term outcome was weak for copeptin (0.62, 95% CI 0.55 to 0.69) and cortisol (0.62, 95% CI 0.54 to 0.69). With logistic regression, admission copeptin (standard deviation (SD) increase OR 1.4, 95% CI 1.03 to 1.98) and cortisol (SD increase OR 1.5, 95% CI 1.1 to 2.0) predicted ICU mortality but not 12-month outcome. Admission factors correlating with SOFA were shockable rhythm (B -1.3, 95% CI -2.2 to -0.5), adrenaline use (B 1.1, 95% CI 0.2 to 2.0), therapeutic hypothermia (B 1.3 95% CI 0.4-2.2), and copeptin (B 0.04, 95% CI 0.02 to 0.07).
Conclusions: Admission copeptin and free cortisol were not of prognostic value regarding 12-month neurological outcome after OHCA. Higher admission copeptin and cortisol were associated with ICU death, and copeptin predicted subsequent organ dysfunction.
Figures
References
-
- Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, et al. Part 9: post-cardiac arrest care American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;2010:S768–86. doi: 10.1161/CIRCULATIONAHA.110.971002. - DOI - PubMed
-
- Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a ‘sepsis-like’ syndrome. Circulation. 2002;106:562–8. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
