

Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: a pilot clinical study
- PMID: 25886857
- PMCID: PMC4403842
- DOI: 10.1186/s13054-015-0894-9
Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: a pilot clinical study
Abstract
Introduction: Pressure-support ventilation, is widely used in critically ill patients; however, the relative contribution of patient's effort during assisted breathing is difficult to measure in clinical conditions. Aim of the present study was to evaluate the performance of ultrasonographic indices of diaphragm contractile activity (respiratory excursion and thickening) in comparison to traditional indices of inspiratory muscle effort during assisted mechanical ventilation.
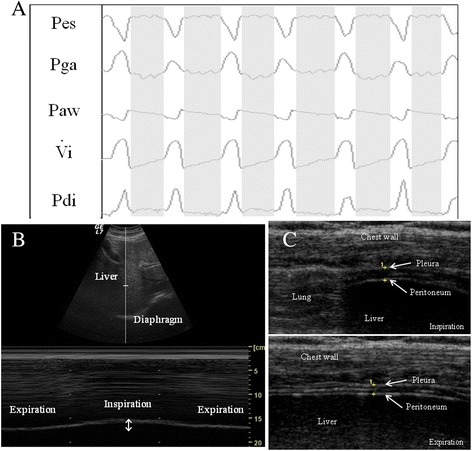
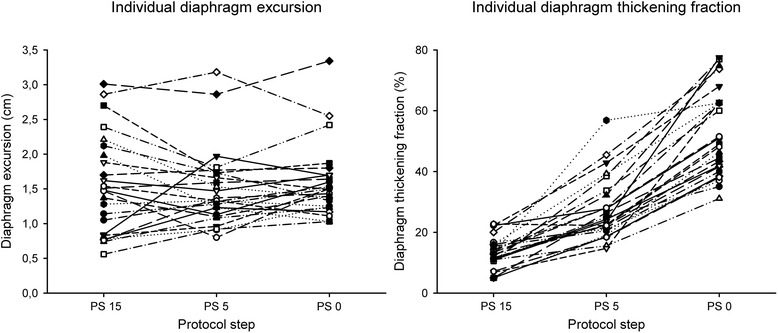
Method: Consecutive patients admitted to the ICU after major elective surgery who met criteria for a spontaneous breathing trial with pressure support ventilation were enrolled. Patients with airflow obstruction or after thoracic/gastric/esophageal surgery were excluded. Variable levels of inspiratory muscle effort were achieved by delivery of different levels of ventilatory assistance by random application of pressure support (0, 5 and 15 cmH2O). The right hemidiaphragm was evaluated by B- and M-mode ultrasonography to record respiratory excursion and thickening. Airway, gastric and oesophageal pressures, and airflow were recorded to calculate indices of respiratory effort (diaphragm and esophageal pressure-time product).
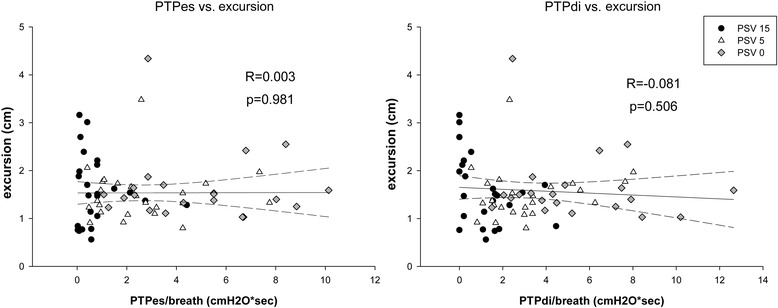
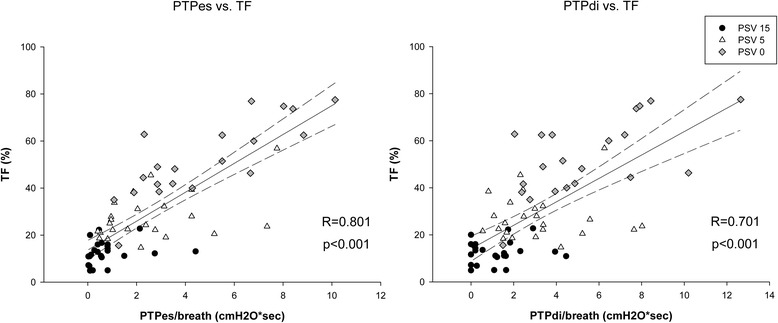
Results: 25 patients were enrolled. With increasing levels of pressure support, parallel reductions were found between diaphragm thickening and both diaphragm and esophageal pressure-time product (respectively, R = 0.701, p < 0.001 and R = 0.801, p < 0.001) during tidal breathing. No correlation was found between either diaphragm or esophageal pressure-time product and diaphragm excursion (respectively, R = -0.081, p = 0.506 and R = 0.003, p = 0.981), nor was diaphragm excursion correlated to diaphragm thickening (R = 0.093, p = 0.450) during tidal breathing.
Conclusions: In patients undergoing in assisted mechanical ventilation, diaphragm thickening is a reliable indicator of respiratory effort, whereas diaphragm excursion should not be used to quantitatively assess diaphragm contractile activity.
Figures
References
-
- Hess DR. Ventilator waveforms and the physiology of pressure support ventilation. Respir Care. 2005;50:166–86. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
