

Implementation and Operational Research: Maternal Combination Antiretroviral Therapy Is Associated With Improved Retention of HIV-Exposed Infants in Kinshasa, Democratic Republic of Congo
- PMID: 25886922
- PMCID: PMC4506694
- DOI: 10.1097/QAI.0000000000000644
Implementation and Operational Research: Maternal Combination Antiretroviral Therapy Is Associated With Improved Retention of HIV-Exposed Infants in Kinshasa, Democratic Republic of Congo
Abstract
Background: Programs to prevent mother-to-child HIV transmission are plagued by loss to follow-up (LTFU) of HIV-exposed infants. We assessed if providing combination antiretroviral therapy (cART) to HIV-infected mothers was associated with reduced LTFU of their HIV-exposed infants in Kinshasa, DR Congo.
Methods: We constructed a cohort of mother-infant pairs using routinely collected clinical data. Maternal cART eligibility was based on national guidelines in effect at the time. Infants were considered LTFU after 3 failed tracking attempts after a missed visit or if more than 6 months passed since they were last seen in clinic. Statistical methods accounted for competing risks (eg, death).
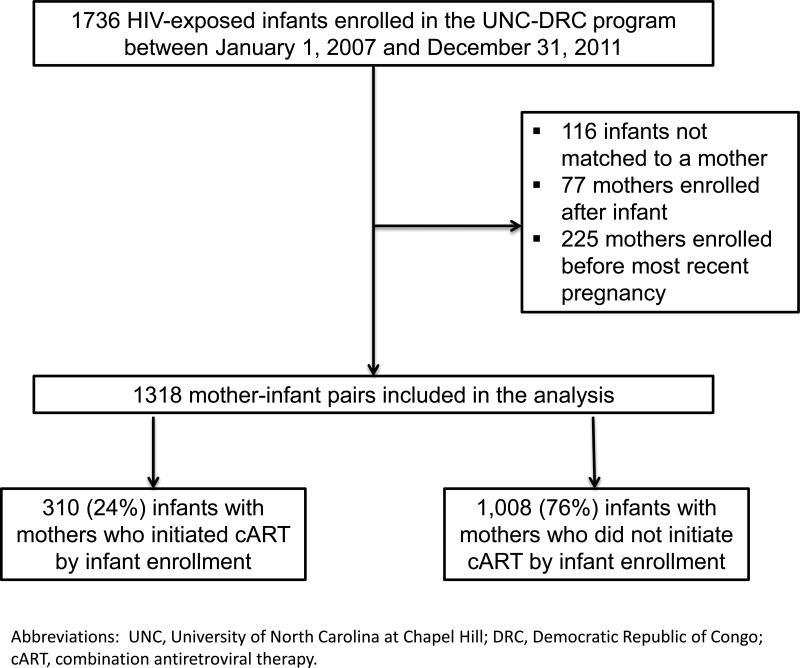
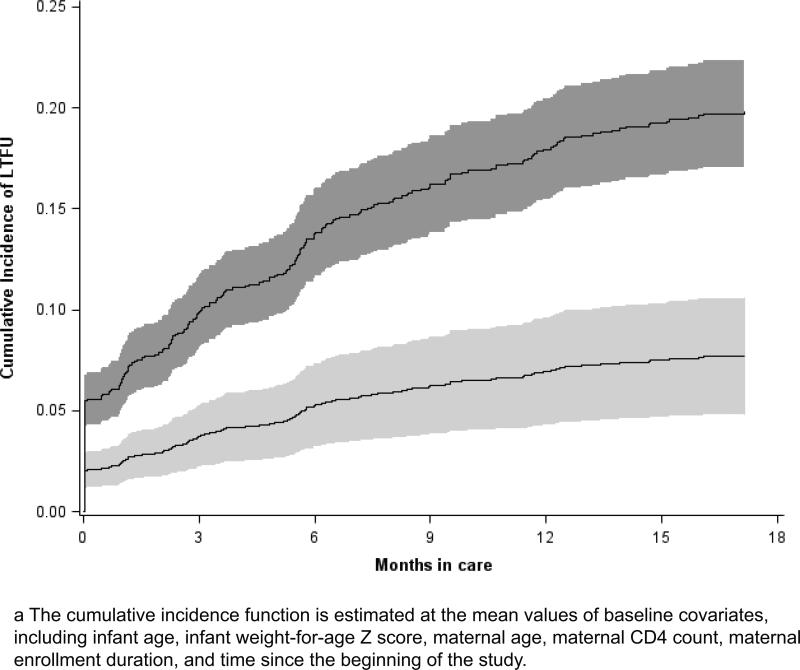
Results: A total of 1318 infants enrolled at a median age of 2.6 weeks (interquartile range: 2.1-6.9), at which point 24% of mothers were receiving cART. Overall, 5% of infants never returned to care after enrollment and 18% were LTFU by 18 months. The 18-month cumulative incidence of LTFU was 8% among infants whose mothers initiated cART by infant enrollment and 20% among infants whose mothers were not yet on cART. Adjusted for baseline factors, infants whose mothers were not on cART were over twice as likely to be LTFU, with a subdistribution hazard ratio of 2.75 (95% confidence limit: 1.81 to 4.16). The association remained strong regardless of maternal CD4 count at infant enrollment.
Conclusions: Increasing access to cART for pregnant women could improve retention of HIV-exposed infants, thereby increasing the clinical and population-level impacts of prevention of mother-to-child HIV transmission interventions and access to early cART for HIV-infected infants.
Figures
Similar articles
-
Temporal changes in the outcomes of HIV-exposed infants in Kinshasa, Democratic Republic of Congo during a period of rapidly evolving guidelines for care (2007-2013).AIDS. 2014 Jul;28 Suppl 3(0 3):S301-11. doi: 10.1097/QAD.0000000000000331. AIDS. 2014. PMID: 24991903 Free PMC article.
-
Loss to Follow-Up within the Prevention of Mother-to-Child Transmission Care Cascade in a Large ART Program in Nigeria.Curr HIV Res. 2015;13(3):201-9. doi: 10.2174/1570162x1303150506183256. Curr HIV Res. 2015. PMID: 25986371 Free PMC article.
-
Triple antiretroviral compared with zidovudine and single-dose nevirapine prophylaxis during pregnancy and breastfeeding for prevention of mother-to-child transmission of HIV-1 (Kesho Bora study): a randomised controlled trial.Lancet Infect Dis. 2011 Mar;11(3):171-80. doi: 10.1016/S1473-3099(10)70288-7. Epub 2011 Jan 13. Lancet Infect Dis. 2011. PMID: 21237718 Clinical Trial.
-
[National consensus document by GESIDA/National Aids Plan on antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2011 update)].Enferm Infecc Microbiol Clin. 2011 Mar;29(3):209.e1-103. doi: 10.1016/j.eimc.2010.12.004. Enferm Infecc Microbiol Clin. 2011. PMID: 21388714 Spanish.
-
Current guidelines for the management of UK Infants born to HIV-1 infected mothers.Early Hum Dev. 2005 Jan;81(1):103-10. doi: 10.1016/j.earlhumdev.2004.10.008. Epub 2004 Nov 19. Early Hum Dev. 2005. PMID: 15707721 Review.
Cited by
-
Firth's Logistic Regression of Interruption in Treatment before and after the Onset of COVID-19 among People Living with HIV on ART in Two Provinces of DRC.Healthcare (Basel). 2022 Aug 12;10(8):1516. doi: 10.3390/healthcare10081516. Healthcare (Basel). 2022. PMID: 36011173 Free PMC article.
-
Practical recommendations for reporting Fine-Gray model analyses for competing risk data.Stat Med. 2017 Nov 30;36(27):4391-4400. doi: 10.1002/sim.7501. Epub 2017 Sep 15. Stat Med. 2017. PMID: 28913837 Free PMC article.
-
Implementation and Operational Research: Decentralization Does Not Assure Optimal Delivery of PMTCT and HIV-Exposed Infant Services in a Low Prevalence Setting.J Acquir Immune Defic Syndr. 2015 Dec 1;70(4):e130-9. doi: 10.1097/QAI.0000000000000781. J Acquir Immune Defic Syndr. 2015. PMID: 26262776 Free PMC article.
-
HIV transmission and retention in care among HIV-exposed children enrolled in Malawi's prevention of mother-to-child transmission programme.J Int AIDS Soc. 2017 Sep 4;20(1):21947. doi: 10.7448/IAS.20.1.21947. J Int AIDS Soc. 2017. PMID: 28884524 Free PMC article.
-
Assessing Option B+ retention and infant follow-up in Lilongwe, Malawi.Int J STD AIDS. 2018 Feb;29(2):185-194. doi: 10.1177/0956462417721658. Epub 2017 Jul 27. Int J STD AIDS. 2018. PMID: 28750577 Free PMC article.
References
-
- The Joint United Nations Programme on HIV/AIDS (UNAIDS) Global report: UNAIDS report on the global AIDS epidemic 2013. UNAIDS; 2013.
-
- World Health Organization (WHO) PMTCT Strategic Vision 2010-2015: Preventing mother-to-child transmission of HIV to reach the UNGASS and Millennium Development Goals: Moving towards the elimination of paediatric HIV. World Health Organization; 2010.
-
- Barker PM, Mphatswe W, Rollins N. Antiretroviral drugs in the cupboard are not enough: the impact of health systems’ performance on mother-to-child transmission of HIV. J Acquir Immune Defic Syndr. 2011;56(2):e45–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
