

Improving Adherence to Antiretroviral Therapy With Triggered Real-time Text Message Reminders: The China Adherence Through Technology Study
- PMID: 25886927
- PMCID: PMC4552400
- DOI: 10.1097/QAI.0000000000000651
Improving Adherence to Antiretroviral Therapy With Triggered Real-time Text Message Reminders: The China Adherence Through Technology Study
Abstract
Background: Real-time adherence monitoring is now possible through medication storage devices equipped with cellular technology. We assessed the effect of triggered cell phone reminders and counseling using objective adherence data on antiretroviral therapy (ART) adherence among Chinese HIV-infected patients.
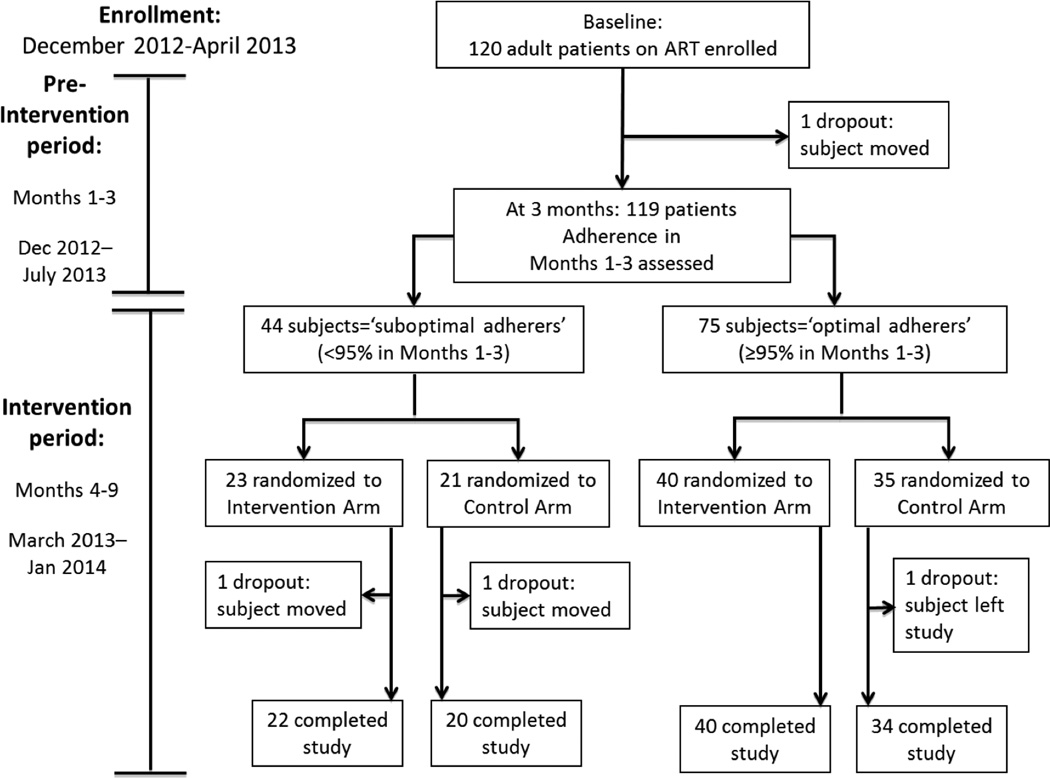
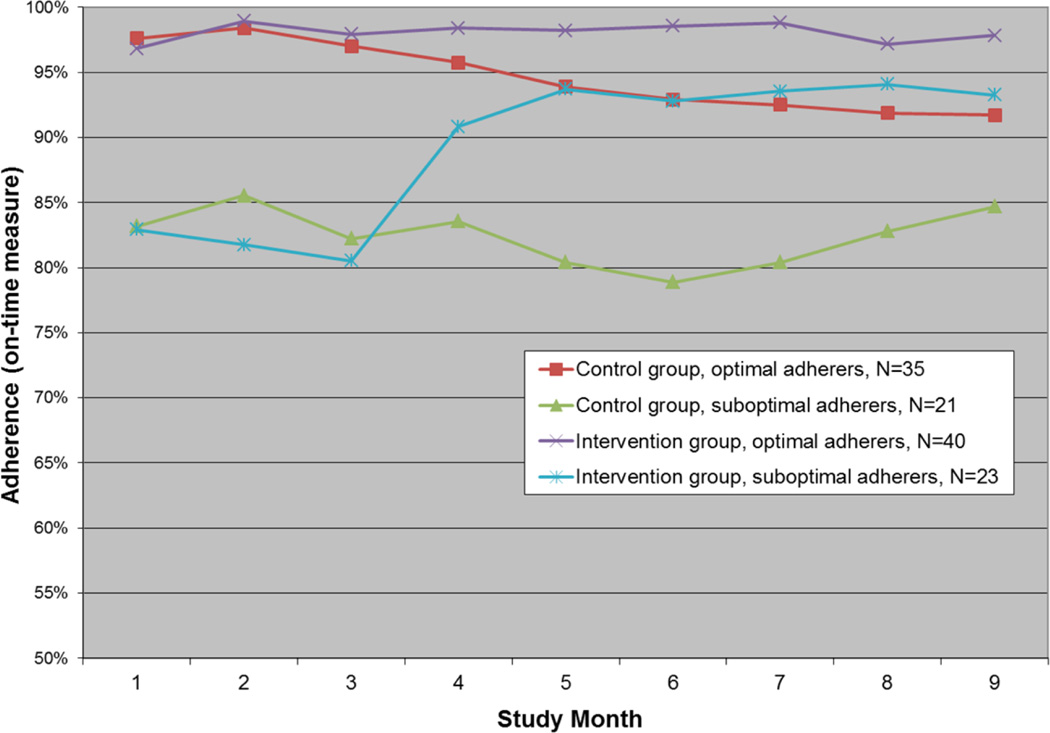
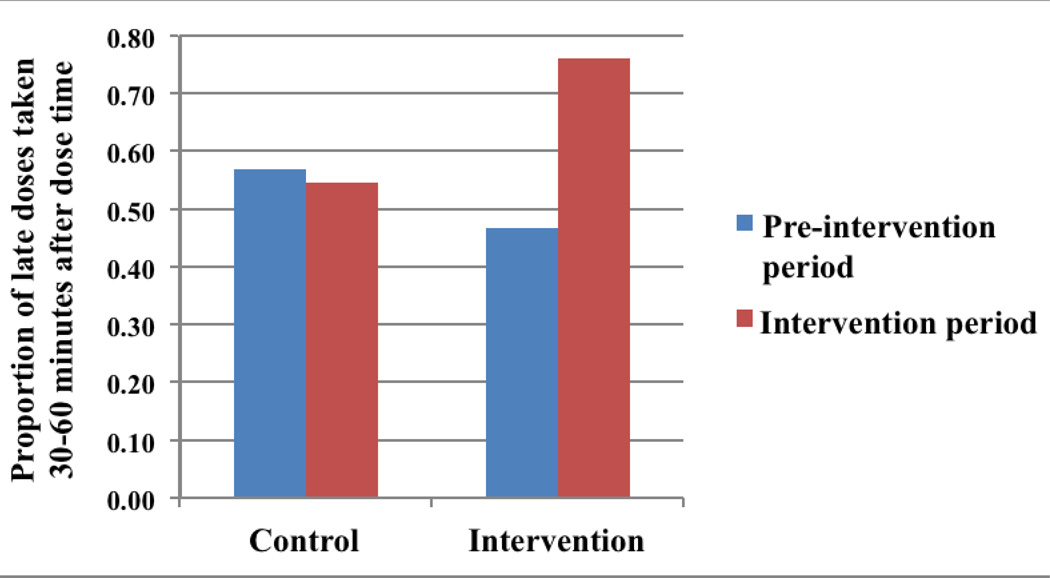
Methods: We provided ART patients in Nanning, China, with a medication device (Wisepill) to monitor their ART adherence electronically. After 3 months, we randomized subjects within optimal (≥95%) and suboptimal (<95%) adherence strata to intervention vs. control arms. In months 4-9, intervention subjects received individualized reminders triggered by late dose taking (no device opening by 30 minutes past dose time) and counseling using device-generated data. Controls received no reminders or data-informed counseling. We compared postintervention proportions achieving optimal adherence, mean adherence, and clinical outcomes.
Results: Of 120 subjects enrolled, 116 (96.7%) completed the trial. Preintervention optimal adherence was similar in intervention vs. control arms (63.5% vs. 58.9%, respectively; P = 0.60). In the last intervention month, 87.3% vs. 51.8% achieved optimal adherence [risk ratio (RR): 1.7, 95% confidence interval (CI): 1.3 to 2.2] and mean adherence was 96.2% vs. 89.1% (P = 0.003). Among preintervention suboptimal adherers, 78.3% vs. 33.3% (RR: 2.4, CI: 1.2 to 4.5) achieved optimal adherence and mean adherence was 93.3% vs. 84.7% (P = 0.039). Proportions were 92.5% and 62.9% among optimal adherers, respectively (RR: 1.5, CI: 1.1 to 1.9) and mean adherence was 97.8% vs. 91.7% (P = 0.028). Postintervention clinical outcomes were not significant.
Conclusions: Real-time reminders significantly improved ART adherence in this population. This approach seems promising for managing HIV and other chronic diseases and warrants further investigation and adaptation in other settings.
Conflict of interest statement
For the remaining authors, no potential conflicts of interest were declared.
Figures
References
-
- UNAIDS. Global Report: UNAIDS Report on the Global AIDS epidemic 2013. Geneva: Joint United Nations Programme on HIV/AIDS; 2013.
-
- Garcia de Olalla P, Knobel H, Carmona A, Guelar A, Lopez-Colomes JL, Cayla JA. Impact of adherence and highly active antiretroviral therapy on survival in HIV-infected patients. J Acquir Immune Defic Syndr. 2002;30(1):105–110. - PubMed
-
- Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. - PubMed
-
- Hogg RS, Heath K, Bangsberg D, et al. Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS. 2002;16(7):1051–1058. - PubMed
-
- Nachega JB, Hislop M, Dowdy DW, et al. Adherence to highly active antiretroviral therapy assessed by pharmacy claims predicts survival in HIV-infected South African adults. J Acquir Immune Defic Syndr. 2006;43(1):78–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
