

Gastric epithelial dysplasia: characteristics and long-term follow-up results after endoscopic resection according to morphological categorization
- PMID: 25886985
- PMCID: PMC4329662
- DOI: 10.1186/s12876-015-0249-7
Gastric epithelial dysplasia: characteristics and long-term follow-up results after endoscopic resection according to morphological categorization
Abstract
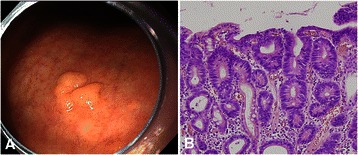
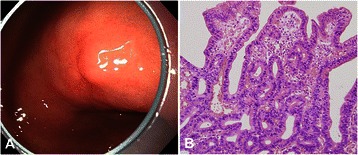
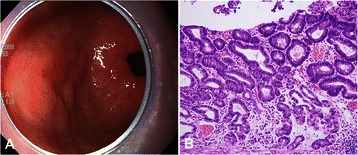
Background: Gastric epithelial dysplasia (GED) can be morphologically categorized into adenomatous and foveolar types. To date, there have been few studies on the clinical characteristics of GEDs according to the morphologic types. Therefore, we here aimed to elucidate the clinicopathologic characteristics of patients with GED and the long-term follow-up results after endoscopic resection according to the morphologic characteristics of GEDs.
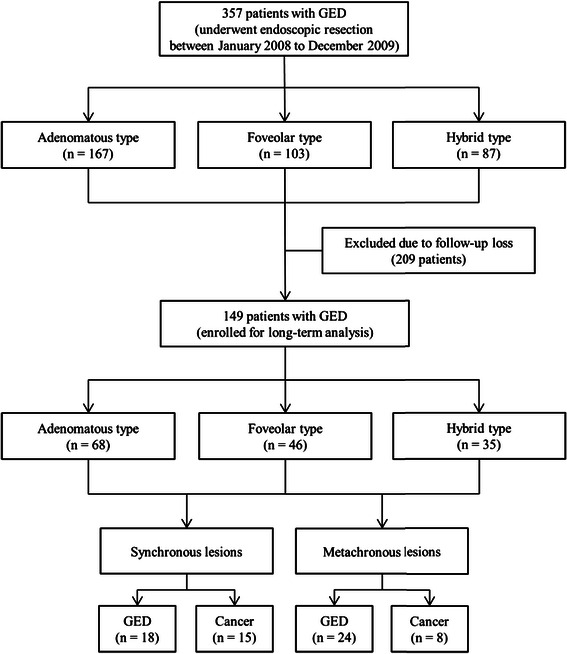
Methods: A total of 357 patients who underwent endoscopic resection for GEDs at Pusan National University Hospital between January 2008 and December 2009 were included in the study. GEDs were morphologically categorized into adenomatous, foveolar, and hybrid types on histologic examination. The clinicopathologic characteristics of patients with GEDs and outcomes of endoscopic resection were analyzed.
Results: Patients with GED were divided into 3 groups: adenomatous (n = 167, 46.8%), foveolar (n = 103, 28.9%), and hybrid (n = 87, 24.3%) types. Compared to the adenomatous type, foveolar type lesions were more frequently located in the antrum/pylorus, flat/depressed lesions, and normal/reddish in color; and showed more frequent high-grade dysplasia. During the follow-up period (median, 37.3 months), the overall incidence of synchronous and metachronous lesions was 20.8% and 20.1%, respectively; of these, the incidence of synchronous and metachronous gastric cancer was 8.7% and 5.4%, respectively. There were no significant differences in the incidence of synchronous and metachronous lesions according to morphologic types.
Conclusion: GEDs appear to have different clinicopathologic characteristics according to morphologic types. Irrespective of the morphology, synchronous and metachronous gastric cancers are commonly found after endoscopic resection of GEDs. Therefore, close follow-up surveillance after endoscopic resection of GEDs should be performed for all patients.
Figures
Similar articles
-
Adenomatous and foveolar gastric dysplasia: distinct patterns of mucin expression and background intestinal metaplasia.Am J Surg Pathol. 2008 Apr;32(4):524-33. doi: 10.1097/PAS.0b013e31815b890e. Am J Surg Pathol. 2008. PMID: 18300795
-
Magnifying endoscopy of gastric epithelial dysplasia based on the morphologic characteristics.World J Gastroenterol. 2014 Nov 14;20(42):15771-9. doi: 10.3748/wjg.v20.i42.15771. World J Gastroenterol. 2014. PMID: 25400462 Free PMC article.
-
Occurrence of metachronous or synchronous lesions after endoscopic treatment of gastric epithelia dysplasia- impact of histologic features of background mucosa.Pathol Res Pract. 2018 Jan;214(1):95-99. doi: 10.1016/j.prp.2017.10.022. Epub 2017 Oct 28. Pathol Res Pract. 2018. PMID: 29103763
-
Synchronous and metachronous gastric adenocarcinoma: case report and literature review.J R Coll Surg Edinb. 1999 Feb;44(1):61-2. J R Coll Surg Edinb. 1999. PMID: 10079673 Review.
-
Diagnosis and management of gastric dysplasia.Korean J Intern Med. 2016 Mar;31(2):201-9. doi: 10.3904/kjim.2016.021. Epub 2016 Feb 26. Korean J Intern Med. 2016. PMID: 26932397 Free PMC article. Review.
Cited by
-
A Systematic Review of the Mechanisms Underlying Treatment of Gastric Precancerous Lesions by Traditional Chinese Medicine.Evid Based Complement Alternat Med. 2020 Apr 26;2020:9154738. doi: 10.1155/2020/9154738. eCollection 2020. Evid Based Complement Alternat Med. 2020. PMID: 32454874 Free PMC article. Review.
-
Risk factors associated with surveillance loss after endoscopic submucosal dissection in patients with gastric neoplasm.Ann Transl Med. 2021 Jul;9(14):1127. doi: 10.21037/atm-21-891. Ann Transl Med. 2021. PMID: 34430568 Free PMC article.
-
Clinical features of gastric adenoma detected within 3 years after negative screening endoscopy in Korea.Gastroenterol Rep (Oxf). 2023 Jul 3;11:goad039. doi: 10.1093/gastro/goad039. eCollection 2023. Gastroenterol Rep (Oxf). 2023. PMID: 37408567 Free PMC article.
-
Identifying the pre-malignant stomach: from guidelines to practice.Transl Gastroenterol Hepatol. 2022 Jan 25;7:8. doi: 10.21037/tgh.2020.03.03. eCollection 2022. Transl Gastroenterol Hepatol. 2022. PMID: 35243117 Free PMC article. Review.
-
Histopathological Evaluation of Gastric Mucosal Atrophy for Predicting Gastric Cancer Risk: Problems and Solutions.Diagnostics (Basel). 2023 Jul 26;13(15):2478. doi: 10.3390/diagnostics13152478. Diagnostics (Basel). 2023. PMID: 37568841 Free PMC article. Review.
References
-
- Correa P. Clinical implications of recent developments in gastric cancer pathology and epidemiology. Semin Oncol. 1985;12:2–10. - PubMed
-
- Rugge M, Farinati F, Baffa R, Sonego F, Di Mario F, Leandro G, et al. Gastric epithelial dysplasia in the natural history of gastric cancer: a multicenter prospective follow-up study, Interdisciplinary Group on Gastric Epithelial Dysplasia. Gastroenterology. 1994;107:1288–96. doi: 10.1016/0016-5085(94)90529-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
