

Hemodynamic consequences of severe lactic acidosis in shock states: from bench to bedside
- PMID: 25887061
- PMCID: PMC4391479
- DOI: 10.1186/s13054-015-0896-7
Hemodynamic consequences of severe lactic acidosis in shock states: from bench to bedside
Erratum in
-
Erratum to: Hemodynamic consequences of severe lactic acidosis in shock states: from bench to bedside.Crit Care. 2017 Feb 21;21(1):40. doi: 10.1186/s13054-017-1624-2. Crit Care. 2017. PMID: 28219394 Free PMC article. No abstract available.
Abstract
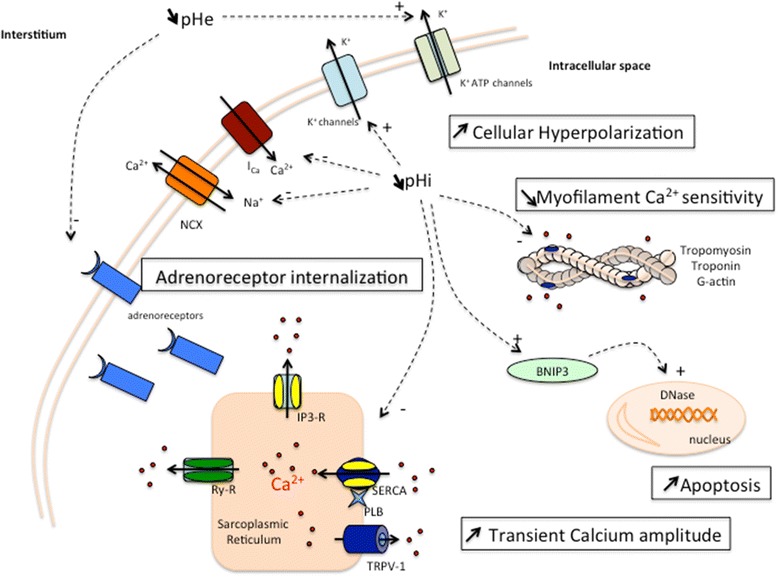
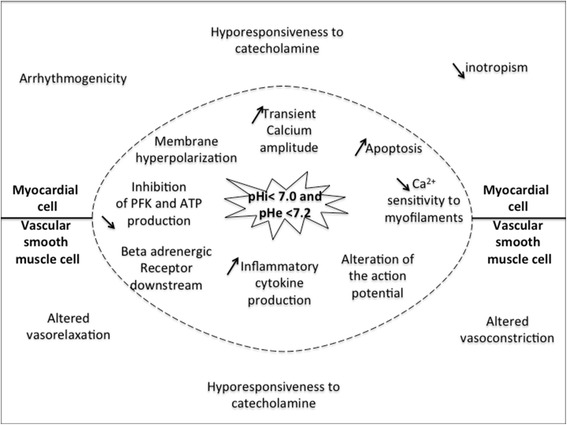
Lactic acidosis is a very common biological issue for shock patients. Experimental data clearly demonstrate that metabolic acidosis, including lactic acidosis, participates in the reduction of cardiac contractility and in the vascular hyporesponsiveness to vasopressors through various mechanisms. However, the contributions of each mechanism responsible for these deleterious effects have not been fully determined and their respective consequences on organ failure are still poorly defined, particularly in humans. Despite some convincing experimental data, no clinical trial has established the level at which pH becomes deleterious for hemodynamics. Consequently, the essential treatment for lactic acidosis in shock patients is to correct the cause. It is unknown, however, whether symptomatic pH correction is beneficial in shock patients. The latest Surviving Sepsis Campaign guidelines recommend against the use of buffer therapy with pH ≥7.15 and issue no recommendation for pH levels <7.15. Furthermore, based on strong experimental and clinical evidence, sodium bicarbonate infusion alone is not recommended for restoring pH. Indeed, bicarbonate induces carbon dioxide generation and hypocalcemia, both cardiovascular depressant factors. This review addresses the principal hemodynamic consequences of shock-associated lactic acidosis. Despite the lack of formal evidence, this review also highlights the various adapted supportive therapy options that could be putatively added to causal treatment in attempting to reverse the hemodynamic consequences of shock-associated lactic acidosis.
Figures
References
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock, 2012. Crit Care Med. 2013;41:580–637. - PubMed
-
- Morris CG, Low J. Metabolic acidosis in the critically ill: part 1. Classification and pathophysiology. Anaesthesia. 2008;63:294–301. - PubMed
-
- Kraut JA, Kurtz I. Use of base in the treatment of acute severe organic acidosis by nephrologists and critical care physicians: results of an online survey. Clin Exp Nephrol. 2006;10:111–7. - PubMed
-
- Noritomi DT, Soriano FG, Kellum JA, Cappi SB, Biselli PJ, Liborio AB, Park M. Metabolic acidosis in patients with severe sepsis and septic shock: a longitudinal quantitative study. Crit Care Med. 2009;37:2733–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
