

Extended-Release Mixed Amphetamine Salts vs Placebo for Comorbid Adult Attention-Deficit/Hyperactivity Disorder and Cocaine Use Disorder: A Randomized Clinical Trial
- PMID: 25887096
- PMCID: PMC4456227
- DOI: 10.1001/jamapsychiatry.2015.41
Extended-Release Mixed Amphetamine Salts vs Placebo for Comorbid Adult Attention-Deficit/Hyperactivity Disorder and Cocaine Use Disorder: A Randomized Clinical Trial
Abstract
Importance: Adult attention-deficit/hyperactivity disorder (ADHD) is prevalent but often unrecognized, in part because it tends to co-occur with other disorders such as substance use disorders. Cocaine use disorder is one such disorder with high co-occurrence of ADHD.
Objective: To examine whether treatment of co-occurring ADHD and cocaine use disorder with extended-release mixed amphetamine salts is effective at both improving ADHD symptoms and reducing cocaine use.
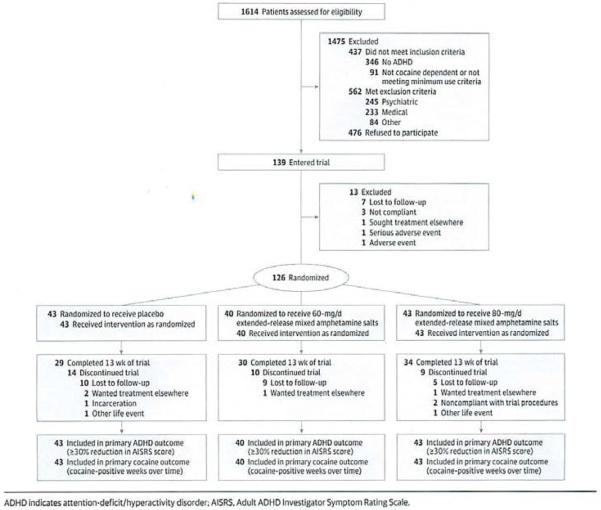
Design, setting, and participants: Thirteen-week, randomized, double-blind, 3-arm, placebo-controlled trial of participants meeting DSM-IV-TR criteria for both ADHD and cocaine use disorder conducted between December 1, 2007, and April 15, 2013, at 2 academic health center substance abuse treatment research sites. One hundred twenty-six adults diagnosed as having comorbid ADHD and cocaine use disorder were randomized to extended-release mixed amphetamine salts or placebo. Analysis was by intent-to-treat population.
Interventions: Participants received extended-release mixed amphetamine salts (60 or 80 mg) or placebo daily for 13 weeks and participated in weekly individual cognitive behavioral therapy.
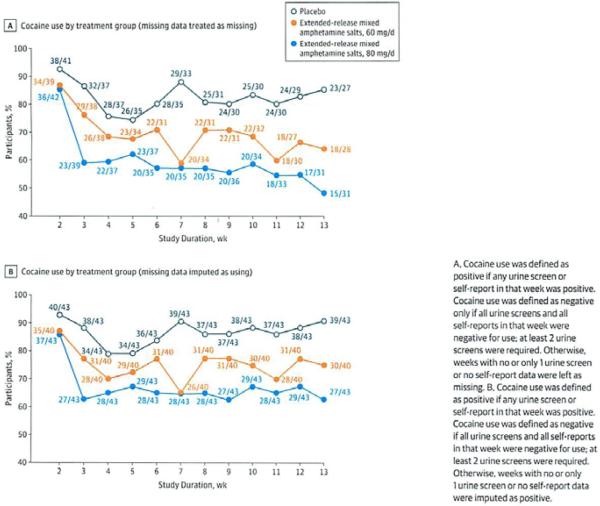
Main outcomes and measures: For ADHD, percentage of participants achieving at least a 30% reduction in ADHD symptom severity, measured by the Adult ADHD Investigator Symptom Rating Scale; for cocaine use, cocaine-negative weeks (by self-report of no cocaine use and weekly benzoylecgonine urine screens) during maintenance medication (weeks 2-13) and percentage of participants achieving abstinence for the last 3 weeks.
Results: More patients achieved at least a 30% reduction in ADHD symptom severity in the medication groups (60 mg: 30 of 40 participants [75.0%]; odds ratio [OR] = 5.23; 95% CI, 1.98-13.85; P < .001; and 80 mg: 25 of 43 participants [58.1%]; OR = 2.27; 95% CI, 0.94-5.49; P = .07) compared with placebo (17 of 43 participants [39.5%]). The odds of a cocaine-negative week were higher in the 80-mg group (OR = 5.46; 95% CI, 2.25-13.27; P < .001) and 60-mg group (OR = 2.92; 95% CI, 1.15-7.42; P = .02) compared with placebo. Rates of continuous abstinence in the last 3 weeks were greater for the medication groups than the placebo group: 30.2% for the 80-mg group (OR = 11.87; 95% CI, 2.25-62.62; P = .004) and 17.5% for the 60-mg group (OR = 5.85; 95% CI, 1.04-33.04; P = .04) vs 7.0% for placebo.
Conclusions and relevance: Extended-release mixed amphetamine salts in robust doses along with cognitive behavioral therapy are effective for treatment of co-occurring ADHD and cocaine use disorder, both improving ADHD symptoms and reducing cocaine use. The data suggest the importance of screening and treatment of ADHD in adults presenting with cocaine use disorder.
Trial registration: clinicaltrials.gov Identifier:NCT00553319.
Figures
References
-
- Barkley RA, Brown TE. Unrecognized attention-deficit/hyperactivity disorder in adults presenting with other psychiatric disorders. CNS Spectr. 2008;13(11):977–984. - PubMed
-
- Biederman J, Wilens T, Mick E, Milberger S, Spencer TJ, Faraone SV. Psychoactive substance use disorders in adults with attention deficit hyperactivity disorder (ADHD): effects of ADHD and psychiatric comorbidity. Am J Psychiatry. 1995;152(11):1652–1658. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
