

A regional trauma system to optimize the pre-hospital triage of trauma patients
- PMID: 25887150
- PMCID: PMC4403891
- DOI: 10.1186/s13054-015-0835-7
A regional trauma system to optimize the pre-hospital triage of trauma patients
Abstract
Introduction: Pre-hospital triage is a key element in a trauma system that aims to admit patients to the most suitable trauma center, and may decrease intra-hospital mortality. We evaluated the performance of a pre-hospital procedure in a regional trauma system through measurements of the quality of pre-hospital medical assessment and the efficacy of a triage protocol.
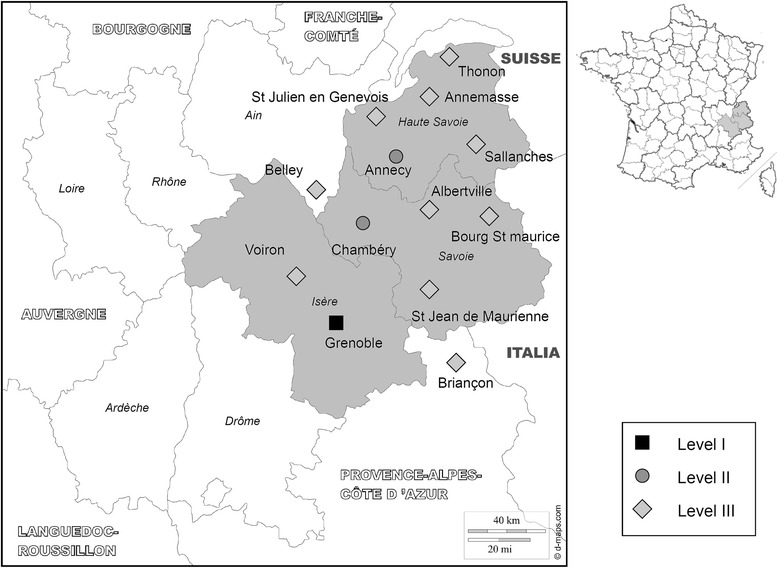
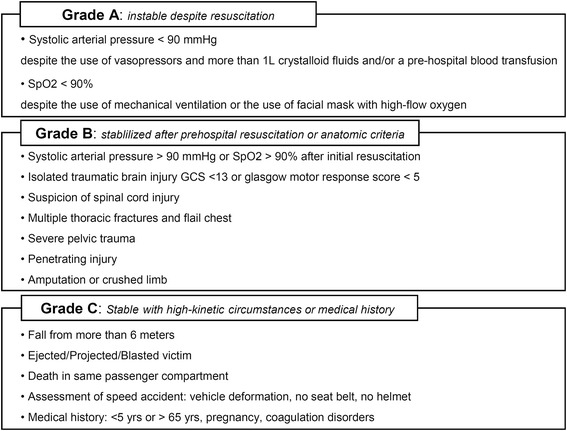
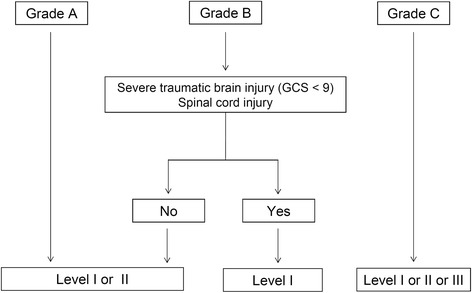
Methods: Our regional trauma system included 13 hospitals categorized as Level I, II or III trauma centers according to their technical facilities. Each patient was graded A, B or C by an emergency physician, according to the seriousness of their injuries at presentation on scene. The triage was performed according to this grading and the categorization of centers. This study is a registry analysis of a three-year period (2009 to 2011).
Results: Of the 3,428 studied patients, 2,572 were graded using the pre-hospital grading system (Graded group). The pre-hospital gradation was closely related with injury severity score (ISS) and intra-hospital mortality rate. The triage protocol had a sensitivity of 92% (95% confidence interval (CI) 90% to 93%) and a specificity of 41% (95% CI 39% to 44%) to predict adequate admission of patients with ISS more than 15. A total of 856 patients were not graded at the scene (Non-graded group). Undertriage rate was significantly reduced in the Graded group compared with the Non-graded group, with a relative risk of 0.47 (95% CI 0.40 to 0.56) according to the definition of the American College of Surgeons Committee on Trauma (P <0.001). Where adjusted for trauma severity, the expected mortality rate at discharge from hospital was higher than observed mortality, with a difference of +2.0% (95% CI 1.4 to 2.6%; P <0.01).
Conclusions: Implementation of a regional trauma system with a pre-hospital triage procedure was effective in detecting severe trauma patients and in lowering the rate of pre-hospital undertriage. A beneficial effect on outcome of such an organization is suggested.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
