

Acute kidney injury after cardiac arrest
- PMID: 25887258
- PMCID: PMC4416259
- DOI: 10.1186/s13054-015-0900-2
Acute kidney injury after cardiac arrest
Abstract
Introduction: The aim of this study was to evaluate the incidence and determinants of AKI in a large cohort of cardiac arrest patients.
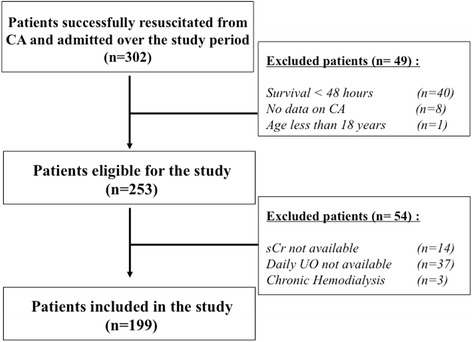
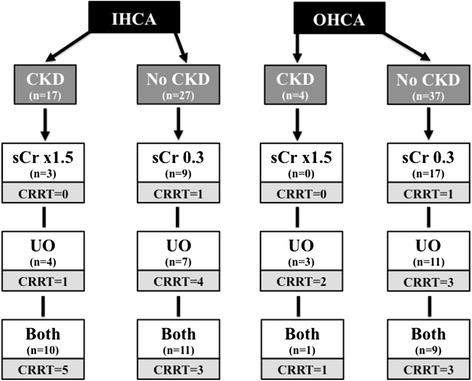
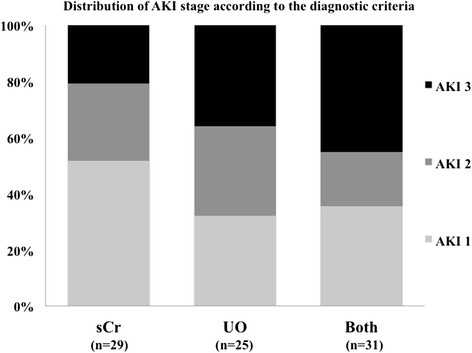
Methods: We reviewed all patients admitted, for at least 48 hours, to our Dept. of Intensive Care after CA between January 2008 and October 2012. AKI was defined as oligo-anuria (daily urine output <0.5 ml/kg/h) and/or an increase in serum creatinine (≥0.3 mg/dl from admission value within 48 hours or a 1.5 time from baseline level). Demographics, comorbidities, CA details, and ICU interventions were recorded. Neurological outcome was assessed at 3 months using the Cerebral Performance Category scale (CPC 1-2 = favorable outcome; 3-5 = poor outcome).
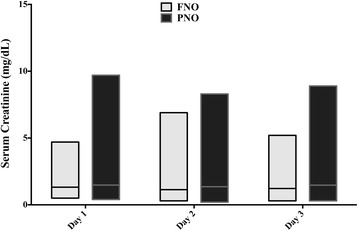
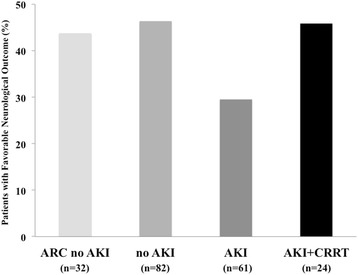
Results: A total of 199 patients were included, 85 (43%) of whom developed AKI during the ICU stay. Independent predictors of AKI development were older age, chronic renal disease, higher dose of epinephrine, in-hospital CA, presence of shock during the ICU stay, a low creatinine clearance (CrCl) on admission and a high cumulative fluid balance at 48 hours. Patients with AKI had higher hospital mortality (55/85 vs. 57/114, p = 0.04), but AKI was not an independent predictor of poor 3-month neurological outcome.
Conclusions: AKI occurred in more than 40% of patients after CA. These patients had more severe hemodynamic impairment and needed more aggressive ICU therapy; however the development of AKI did not influence neurological recovery.
Figures
References
-
- Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–83 - PubMed
-
- Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106:562–8. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
-
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–10. doi: 10.1007/BF01709751. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
