

Characterization of the extent of a large outbreak of Legionnaires' disease by serological assays
- PMID: 25887275
- PMCID: PMC4383209
- DOI: 10.1186/s12879-015-0903-2
Characterization of the extent of a large outbreak of Legionnaires' disease by serological assays
Abstract
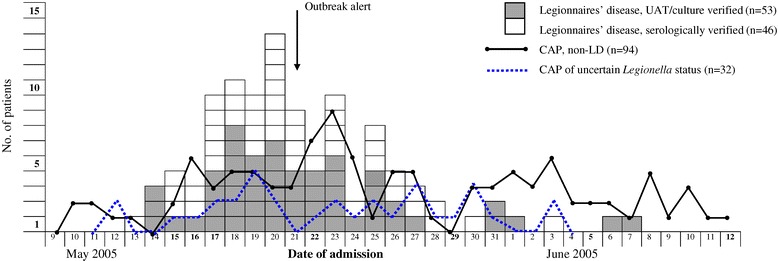
Background: In May 2005, a long-distance outbreak of Legionnaires' disease (LD) caused by Legionella pneumophila serogroup 1 occurred in south-east Norway. The initial outbreak investigation without serology identified 56 laboratory-confirmed LD cases of whom 10 died. However, 116 patients with community-acquired pneumonia might belong to the outbreak based on epidemiological investigations, but acute laboratory tests other than serology were negative or not performed. To assess the true extent of the outbreak, we evaluated two serological assays in order to reclassify the 116 patients with indeterminate case status.
Methods: Two polyvalent antibody tests, a serogroup 1-6 immunofluorescence assay (IFA) and a serogroup 1-7 enzyme-linked immunosorbent assay (ELISA) were used. They were evaluated with cases defined as culture- or urinary antigen positive LD patients (n=40) and non-cases defined as confirmed non-LD patients (n=39) and healthy control subjects (n=62). The 116 patients, who were negative in culture, polymerase chain reaction and/or urinary antigen tests, were analysed by the same serological assays. Antibodies to the outbreak strain were determined by immunoblotting.
Results: In the evaluation study, the sensitivity and specificity of a ≥4-fold IFA titre change was 38% and 100%, respectively, with corresponding values of 30% and 99% for seroconversion in ELISA. A single high positive IFA titre yielded sensitivity and specificity of 73% and 97%, respectively, with corresponding values of 68% and 96% for a single high immunoglobulin (Ig) G and/or IgM in ELISA. Based on this evaluation, the following serological testing identified 47 more LD cases, and the outbreak thus comprised 103 cases with a case fatality rate of 10%. About the same proportion (70%) of the urinary antigen positive and negative LD cases had antibodies to the serogroup-specific lipopolysaccharide of the outbreak strain. In addition to the 103 LD cases, Legionella infection could not be verified or excluded in 32 patients based on epidemiology and/or lack of microbiological sampling.
Conclusions: The acute-phase tests (culture, polymerase chain reaction, and urinary antigen) identified less than 55% of the 103 patients in this outbreak. Serological testing thus remains an important supplement for diagnosis of LD and for determination of outbreak cases.
Figures


References
-
- Norwegian Surveillance System for Communicable Diseases (MSIS). [http://www.msis.no]
-
- Ricketts KD, Joseph CA, European Working Group for Legionella Infections Legionnaires disease’ in Europe: 2005–2006. Euro Surveill. 2007;12:E7–8. - PubMed
-
- Garasen H, Sagvik E, Kvendbo JF, Lian A, Jacobsen T, Nylenna M. Legionella in Trondheim, Norway – determining sources of contagion and tracing risk environments. Tidsskr Nor Laegeforen. 2005;125:1791–3. - PubMed
-
- Marston BJ, Plouffe JF, File TM, Jr, Hackman BA, Salstrom SJ, Lipman HB, et al. Incidence of community-acquired pneumonia requiring hospitalization. Results of a population-based active surveillance Study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med. 1997;157:1709–18. doi: 10.1001/archinte.1997.00440360129015. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
