

Single administration of intra-articular bupivacaine in arthroscopic knee surgery: a systematic review and meta-analysis
- PMID: 25887534
- PMCID: PMC4328055
- DOI: 10.1186/s12891-015-0477-6
Single administration of intra-articular bupivacaine in arthroscopic knee surgery: a systematic review and meta-analysis
Abstract
Background: Single administration of intra-articular (IA) bupivacaine for pain relief after arthroscopic knee surgery is effective, but its active duration and dose-response relationship is unclear. We conducted this meta-analysis to summarize all published randomized controlled trials (RCTs), thus providing the most recent information on the safety and efficacy of single-administration IA bupivacaine for pain relief after arthroscopic knee surgery, and to determine whether a dose-response relationship exists.
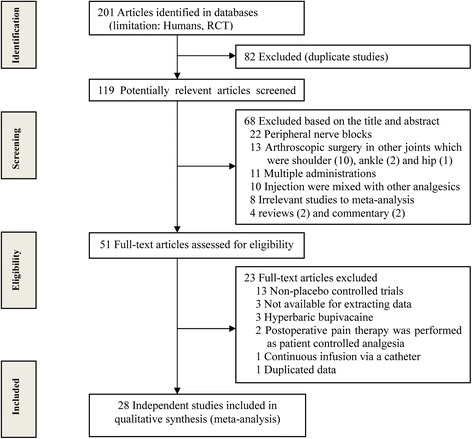
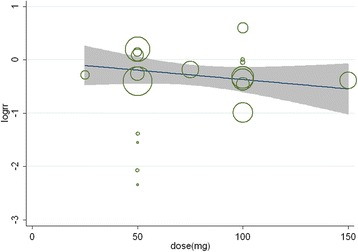
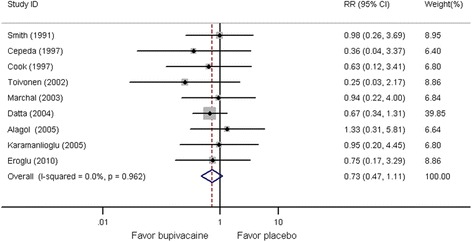
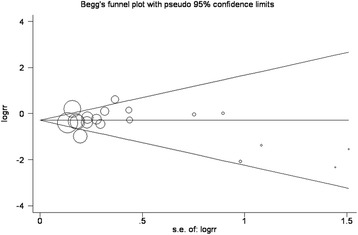
Methods: A systematic electronic literature search (through April 2014) was conducted to identify those RCTs that addressed the safety and efficacy of a single administration of IA bupivacaine for pain management after arthroscopic knee surgery. Subgroup analysis was conducted to determine changes in visual analog scale (VAS) scores at seven postoperative time points. Meta-regression and subgroup analyses were carried out to assess the effects of various treatment factors on efficacy and to evaluate the dose-response relationship of bupivacaine. Weighted mean differences or relative risks were calculated and pooled using a random-effects model.
Results: Twenty-eight trials involving 1,560 patients who underwent arthroscopic knee surgery met the inclusion criteria. The trials were subject to medium risk of bias. VAS scores at 2, 4, 6, 12, and 24 h postoperatively were significantly lower, the number of patients requiring supplementary analgesia was smaller, and the time to first request for analgesia was longer in the IA bupivacaine group than in the placebo group. The analgesic effect of single-administration IA bupivacaine may be associated with the effect of concomitant administration of epinephrine and concentration of bupivacaine, and no dose-response relationship was identified. No significant difference in side effects was detected between groups.
Conclusions: Current evidence shows that the use of single-administration IA bupivacaine is effective for postoperative pain management in patients undergoing arthroscopic knee surgery, with satisfactory short-term safety. Low-dose administration of IA bupivacaine 0.5% combined with epinephrine adjuvant in clinical practice should be performed. Additional high-quality RCTs with longer follow-up periods are required to examine the safety of single-administration IA bupivacaine.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
