

Mass campaigns with antimalarial drugs: a modelling comparison of artemether-lumefantrine and DHA-piperaquine with and without primaquine as tools for malaria control and elimination
- PMID: 25887935
- PMCID: PMC4376519
- DOI: 10.1186/s12879-015-0887-y
Mass campaigns with antimalarial drugs: a modelling comparison of artemether-lumefantrine and DHA-piperaquine with and without primaquine as tools for malaria control and elimination
Abstract
Background: Antimalarial drugs are a powerful tool for malaria control and elimination. Artemisinin-based combination therapies (ACTs) can reduce transmission when widely distributed in a campaign setting. Modelling mass antimalarial campaigns can elucidate how to most effectively deploy drug-based interventions and quantitatively compare the effects of cure, prophylaxis, and transmission-blocking in suppressing parasite prevalence.
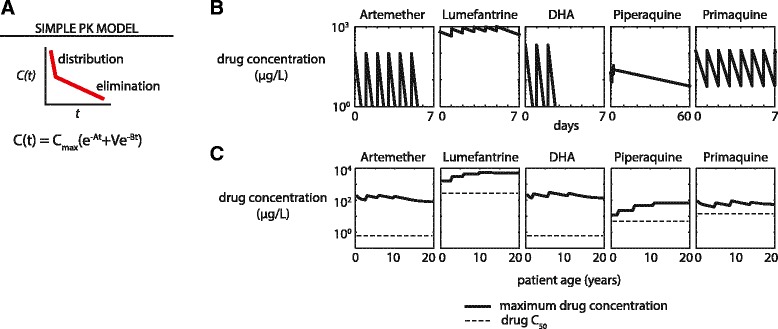
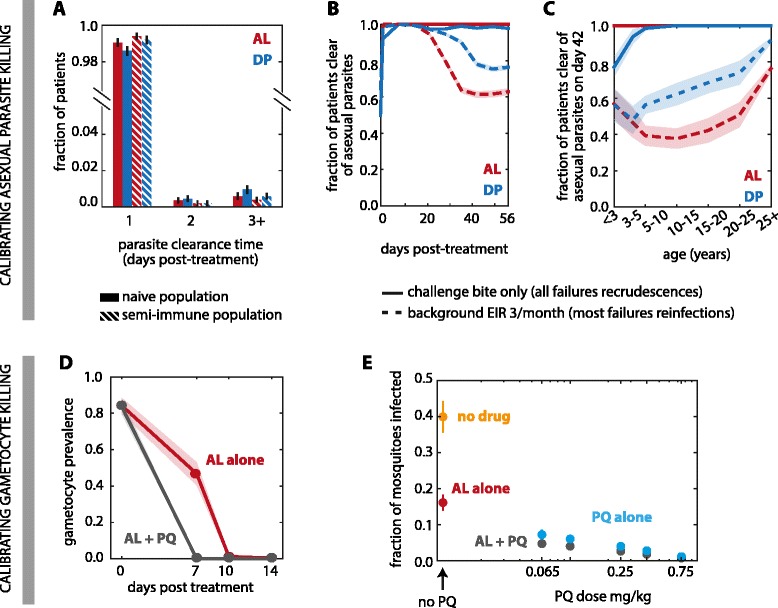
Methods: A previously established agent-based model that includes innate and adaptive immunity was used to simulate malaria infections and transmission. Pharmacokinetics of artemether, lumefantrine, dihydroartemisinin, piperaquine, and primaquine were modelled with a double-exponential distribution-elimination model including weight-dependent parameters and age-dependent dosing. Drug killing of asexual parasites and gametocytes was calibrated to clinical data. Mass distribution of ACTs and primaquine was simulated with seasonal mosquito dynamics at a range of transmission intensities.
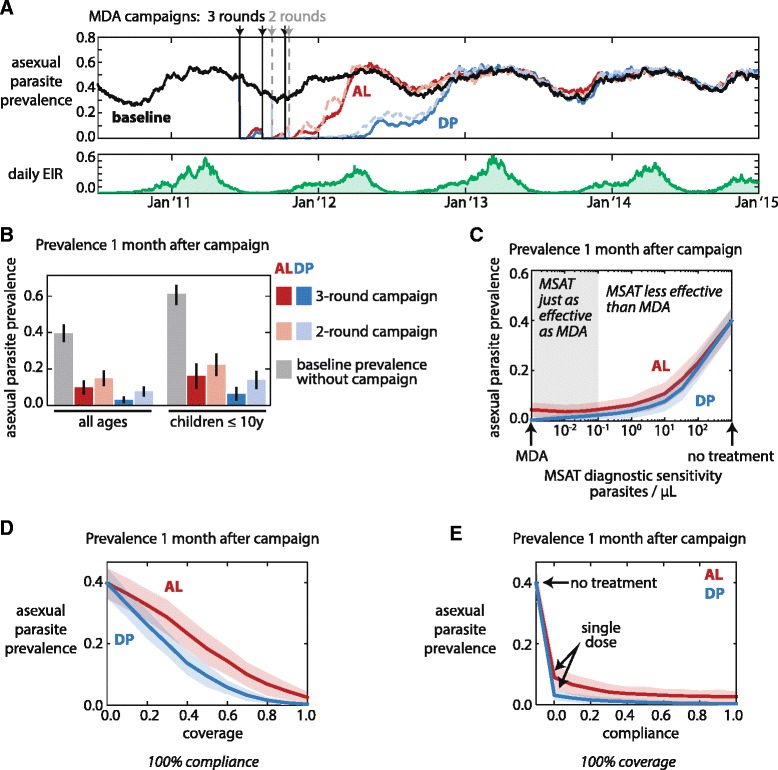
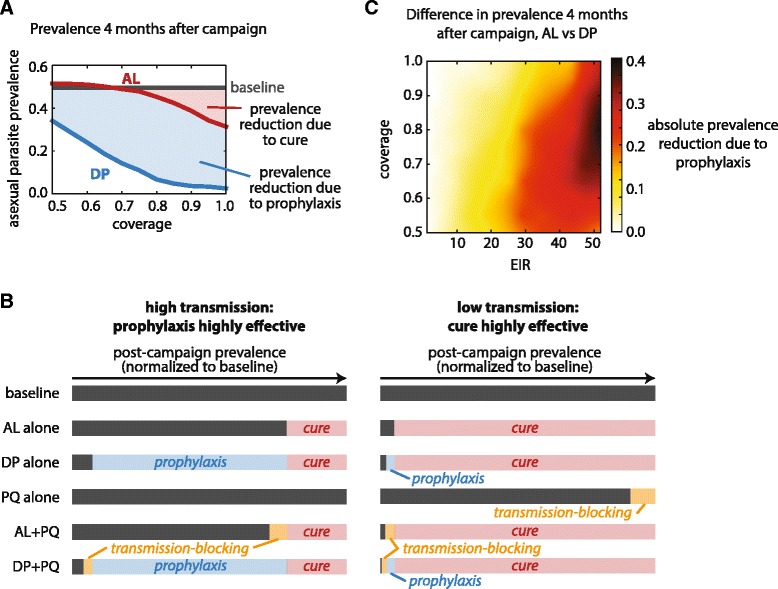
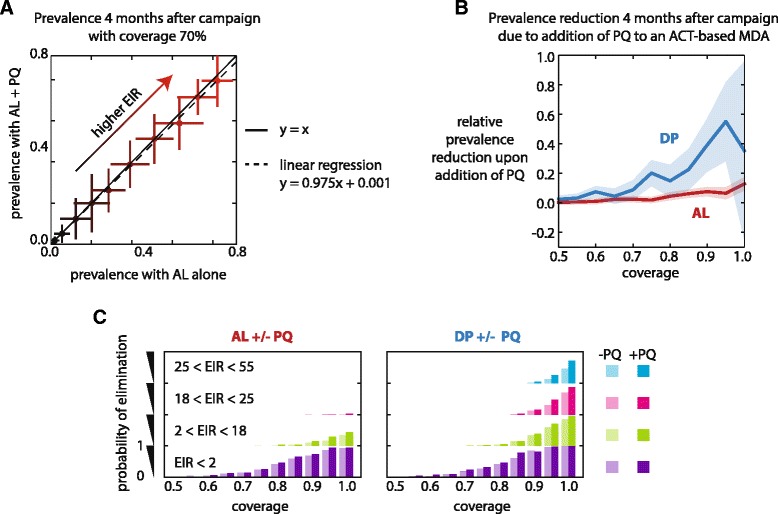
Results: A single mass campaign with antimalarial drugs is insufficient to permanently reduce malaria prevalence when transmission is high. Current diagnostics are insufficiently sensitive to accurately identify asymptomatic infections, and mass-screen-and-treat campaigns are much less efficacious than mass drug administrations. Improving campaign coverage leads to decreased prevalence one month after the end of the campaign, while increasing compliance lengthens the duration of protection against reinfection. Use of a long-lasting prophylactic as part of a mass drug administration regimen confers the most benefit under conditions of high transmission and moderately high coverage. Addition of primaquine can reduce prevalence but exerts its largest effect when coupled with a long-lasting prophylactic.
Conclusions: Mass administration of antimalarial drugs can be a powerful tool to reduce prevalence for a few months post-campaign. A slow-decaying prophylactic administered with a parasite-clearing drug offers strong protection against reinfection, especially in highly endemic areas. Transmission-blocking drugs have only limited effects unless administered with a prophylactic under very high coverage.
Figures
References
-
- World Health Organization . World Malaria Report 2013. Geneva: WHO; 2013.
-
- Greenwood B. The use of anti-malarial drugs to prevent malaria in the population of malaria-endemic areas. Am J Trop Med Hyg. 2004;70:1–7. - PubMed
-
- von Seidlein L, Walraven G, Milligan PJ, Alexander N, Manneh F, Deen JL, et al. The effect of mass administration of sulfadoxine-pyrimethamine combined with artesunate on malaria incidence: a double-blind, community-randomized, placebo-controlled trial in The Gambia. Trans R Soc Trop Med Hyg. 2003;97:217–225. doi: 10.1016/S0035-9203(03)90125-8. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
