

Increasing the inspiratory time and I:E ratio during mechanical ventilation aggravates ventilator-induced lung injury in mice
- PMID: 25888164
- PMCID: PMC4336519
- DOI: 10.1186/s13054-015-0759-2
Increasing the inspiratory time and I:E ratio during mechanical ventilation aggravates ventilator-induced lung injury in mice
Abstract
Introduction: Lung-protective ventilation reduced acute respiratory distress syndrome (ARDS) mortality. To minimize ventilator-induced lung injury (VILI), tidal volume is limited, high plateau pressures are avoided, and positive end-expiratory pressure (PEEP) is applied. However, the impact of specific ventilatory patterns on VILI is not well defined. Increasing inspiratory time and thereby the inspiratory/expiratory ratio (I:E ratio) may improve oxygenation, but may also be harmful as the absolute stress and strain over time increase. We thus hypothesized that increasing inspiratory time and I:E ratio aggravates VILI.
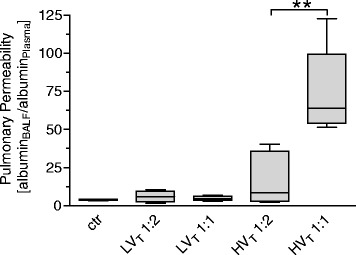
Methods: VILI was induced in mice by high tidal-volume ventilation (HVT 34 ml/kg). Low tidal-volume ventilation (LVT 9 ml/kg) was used in control groups. PEEP was set to 2 cm H2O, FiO2 was 0.5 in all groups. HVT and LVT mice were ventilated with either I:E of 1:2 (LVT 1:2, HVT 1:2) or 1:1 (LVT 1:1, HVT 1:1) for 4 hours or until an alternative end point, defined as mean arterial blood pressure below 40 mm Hg. Dynamic hyperinflation due to the increased I:E ratio was excluded in a separate group of animals. Survival, lung compliance, oxygenation, pulmonary permeability, markers of pulmonary and systemic inflammation (leukocyte differentiation in lung and blood, analyses of pulmonary interleukin-6, interleukin-1β, keratinocyte-derived chemokine, monocyte chemoattractant protein-1), and histopathologic pulmonary changes were analyzed.
Results: LVT 1:2 or LVT 1:1 did not result in VILI, and all individuals survived the ventilation period. HVT 1:2 decreased lung compliance, increased pulmonary neutrophils and cytokine expression, and evoked marked histologic signs of lung injury. All animals survived. HVT 1:1 caused further significant worsening of oxygenation, compliance and increased pulmonary proinflammatory cytokine expression, and pulmonary and blood neutrophils. In the HVT 1:1 group, significant mortality during mechanical ventilation was observed.
Conclusion: According to the "baby lung" concept, mechanical ventilation-associated stress and strain in overinflated regions of ARDS lungs was simulated by using high tidal-volume ventilation. Increase of inspiratory time and I:E ratio significantly aggravated VILI in mice, suggesting an impact of a "stress/strain × time product" for the pathogenesis of VILI. Thus increasing the inspiratory time and I:E ratio should be critically considered.
Figures








References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
