

Incidence and outcome of inappropriate in-hospital empiric antibiotics for severe infection: a systematic review and meta-analysis
- PMID: 25888181
- PMCID: PMC4358713
- DOI: 10.1186/s13054-015-0795-y
Incidence and outcome of inappropriate in-hospital empiric antibiotics for severe infection: a systematic review and meta-analysis
Abstract
Introduction: The aims of this study were to explore the incidence of in-hospital inappropriate empiric antibiotic use in patients with severe infection and to identify its relationship with patient outcomes.
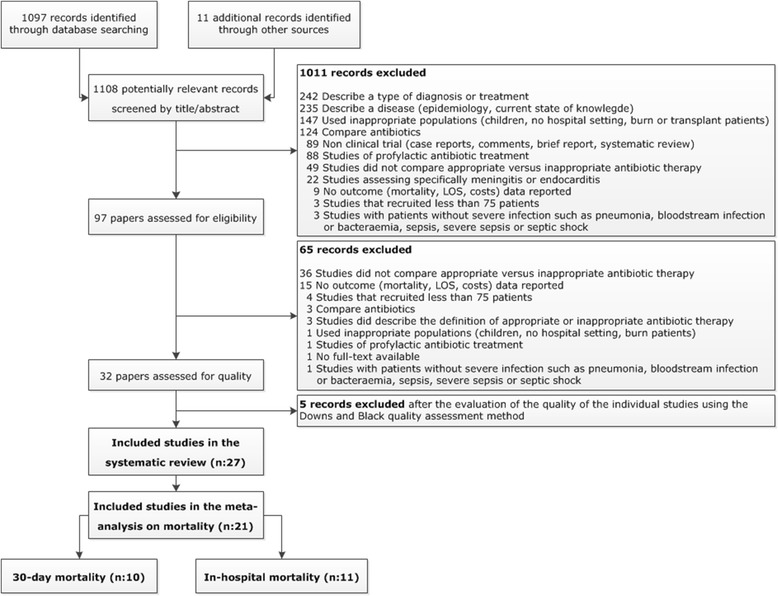
Methods: Medline (from 2004 to 2014) was systematically searched by using predefined inclusion criteria. Reference lists of retrieved articles were screened for additional relevant studies. The systematic review included original articles reporting a quantitative measure of the association between the use of (in)appropriate empiric antibiotics in patients with severe in-hospital infections and their outcomes. A meta-analysis, using a random-effects model, was conducted to quantify the effect on mortality by using risk ratios.
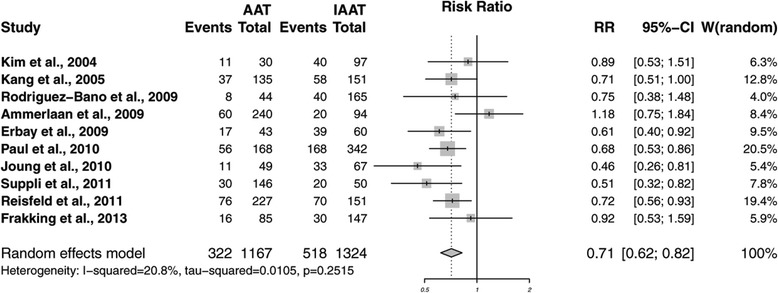
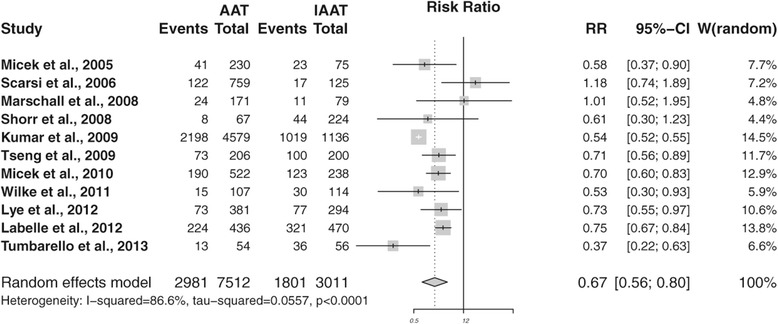
Results: In total, 27 individual articles fulfilled the inclusion criteria. The percentage of inappropriate empiric antibiotic use ranged from 14.1% to 78.9% (Q1-Q3: 28.1% to 57.8%); 13 of 27 studies (48.1%) described an incidence of 50% or more. A meta-analysis for 30-day mortality and in-hospital mortality showed risk ratios of 0.71 (95% confidence interval 0.62 to 0.82) and 0.67 (95% confidence interval 0.56 to 0.80), respectively. Studies with outcome parameter 28-day and 60-day mortality reported significantly (P ≤0.02) higher mortality rates in patients receiving inappropriate antibiotics. Two studies assessed the total costs, which were significantly higher in both studies (P ≤0.01).
Conclusions: This systematic review with meta-analysis provides evidence that inappropriate use of empiric antibiotics increases 30-day and in-hospital mortality in patients with a severe infection.
Figures
References
-
- World Health Organization. World health statistics 2012. http://www.who.int/gho/publications/world_health_statistics/EN_WHS2012_F.... Accessed March 9, 2015.
-
- Heron M, Hoyert S, Murphy J, Kochanek K, Tejada-Vera B. Deaths: final data for 2006. Division of Vital Statistics, Centers for Disease Control and Prevention. Natl Vital Stat Rep. 2009;57:1–136. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
