

High central venous saturation after cardiac surgery is associated with increased organ failure and long-term mortality: an observational cross-sectional study
- PMID: 25888321
- PMCID: PMC4415351
- DOI: 10.1186/s13054-015-0889-6
High central venous saturation after cardiac surgery is associated with increased organ failure and long-term mortality: an observational cross-sectional study
Abstract
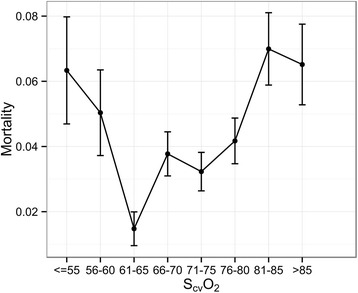
Introduction: Central venous saturation (ScvO2) monitoring has been suggested to address the issue of adequate cardiocirculatory function in the context of cardiac surgery. The aim of this study was to determine the impact of low (L) (<60%), normal (N) (60%-80%), and high (H) (>80%) ScvO2 measured on intensive care unit (ICU) admission after cardiac surgery.
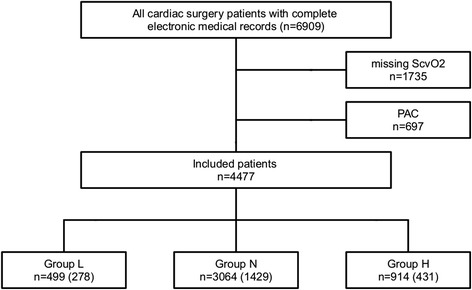
Methods: We conducted a retrospective, cross-sectional, observational study at three ICUs of a university hospital department for anaesthesiology and intensive care. Electronic patient records of all adults who underwent cardiac surgery between 2006 and 2013 and available admission measurements of ScvO2 were examined. Patients were allocated to one of three groups according to first ScvO2 measurement after ICU admission: group L (<60%), group N (60%-80%), and group H (>80%). Primary end-points were in-hospital and 3-year follow-up survival.
Results: Data from 4,447 patients were included in analysis. Low and high initial measurements of ScvO2 were associated with increased in-hospital mortality (L: 5.6%; N: 3.3%; H: 6.8%), 3-year follow-up mortality (L: 21.6%; N: 19.3%; H: 25.8%), incidence of post-operative haemodialysis (L: 11.5%; N: 7.8%; H: 15.3%), and prolonged hospital length of stay (L: 13 days, 9-22; N: 12 days, 9-19; H: 14 days, 9-21). After adjustment for possible confounding variables, an initial ScvO2 above 80% was associated with adjusted hazard ratios of 2.79 (95% confidence interval (CI) 1.565-4.964, P <0.001) for in-hospital survival and 1.31 (95% CI 1.033-1.672, P = 0.026) for 3-year follow-up survival.
Conclusions: Patients with high ScvO2 were particularly affected by unfavourable outcomes. Advanced haemodynamic monitoring may help to identify patients with high ScvO2 who developed extraction dysfunction and to establish treatment algorithms to improve patient outcome in these patients.
Figures

Comment in
-
Alleviating central venous oxygen saturation (ScvO2): a new approach of kidney protection after cardiac surgery?Crit Care. 2015 Oct 21;19:359. doi: 10.1186/s13054-015-1079-2. Crit Care. 2015. PMID: 26486127 Free PMC article. No abstract available.
-
Authors' response.Crit Care. 2015;19:359. Crit Care. 2015. PMID: 26630699 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
