

Excretion of urinary histamine and N-tele methylhistamine in patients with gastrointestinal food allergy compared to non-allergic controls during an unrestricted diet and a hypoallergenic diet
- PMID: 25888445
- PMCID: PMC4389952
- DOI: 10.1186/s12876-015-0268-4
Excretion of urinary histamine and N-tele methylhistamine in patients with gastrointestinal food allergy compared to non-allergic controls during an unrestricted diet and a hypoallergenic diet
Abstract
Background: Patients with gastrointestinal food allergy are characterised by increased production of mast cell derived mediators upon allergen contact and present often with unspecific symptoms. The aim of this study was to evaluate urinary histamine and methylhistamine excretion in patients with food allergy and to compare their values with food-tolerant controls.
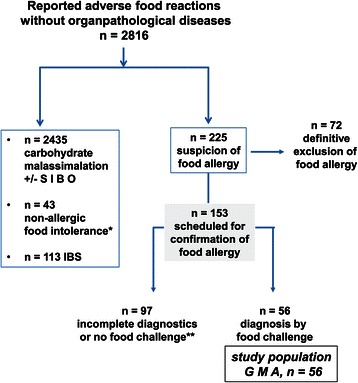
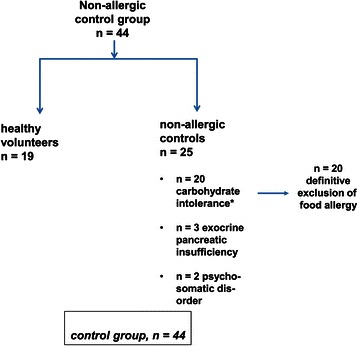
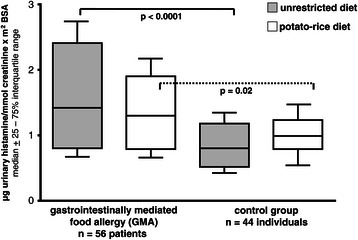
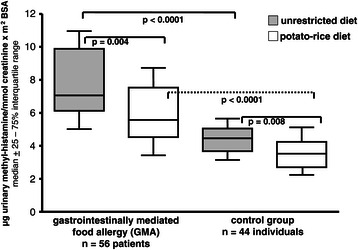
Methods: In a retrospective case control study the urinary excretion parameters were analysed from 56 patients (40.9, 19 - 58 years) in whom later food challenge tests confirmed food allergy. During their diagnostic work-up urine was collected during a 12-h period under an unrestricted diet with staple foods and a hypoallergenic potato-rice-diet (each 2 days). Healthy controls underwent the same diet types to define normal excretion parameters. Urinary histamine and n-methylhistamine were determined by ELISA or tandem mass spectrometry, respectively, and were expressed as median (25 - 75% range, μg/mmol creatinine x m(2)BSA).
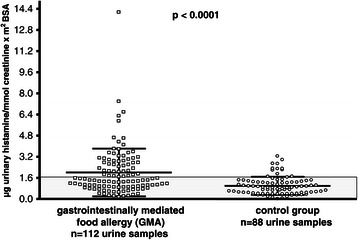
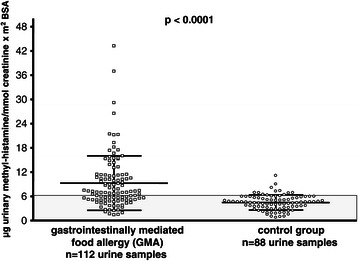
Results: During unrestricted diet urinary histamine was significantly higher in gastrointestinal food allergy than healthy controls (1.42, 0.9 - 2.7 vs 0.87, 0.4 - 1.3; p < 0.0001), while the difference between both groups became marginal during potato-rice diet (1.30, 0.7 - 2.1 vs 1.05, 0.5 - 1.5; p = 0.02). N-methylhistamine was found to be significantly elevated in gastrointestinal food allergy both during unrestricted diet (7.1, 5.0 - 11.2) and potato-rice diet (5.7, 3.7 - 8.7) compared to controls (p < 0.0001). Interestingly, urinary methylhistamine excretion (p < 0.004) and clinical symptom score (p < 0.02) fell significantly when the diet was switched from unrestricted to hypoallergenic food, but was not correlated with symptom scores.
Conclusions: In gastrointestinal food allergy significantly higher levels of urine histamine and methylhistamine excretion were found under unrestricted diet, reflecting an increased secretion of histamine due to offending foods. Measurement of urinary n-methylhistamine levels may help to find out patients with increased histamine production and/or food-allergen induced clinical symptoms, respectively.
Figures
Comment in
-
[Food allergies: urine test can provide information].Dtsch Med Wochenschr. 2015 May;140(10):707. doi: 10.1055/s-0041-101822. Dtsch Med Wochenschr. 2015. PMID: 26171470 German. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
