

Neighbourhood immigration, health care utilization and outcomes in patients with diabetes living in the Montreal metropolitan area (Canada): a population health perspective
- PMID: 25888912
- PMCID: PMC4422525
- DOI: 10.1186/s12913-015-0824-1
Neighbourhood immigration, health care utilization and outcomes in patients with diabetes living in the Montreal metropolitan area (Canada): a population health perspective
Abstract
Background: Understanding health care utilization by neighbourhood is essential for optimal allocation of resources, but links between neighbourhood immigration and health have rarely been explored. Our objective was to understand how immigrant composition of neighbourhoods relates to health outcomes and health care utilization of individuals living with diabetes.
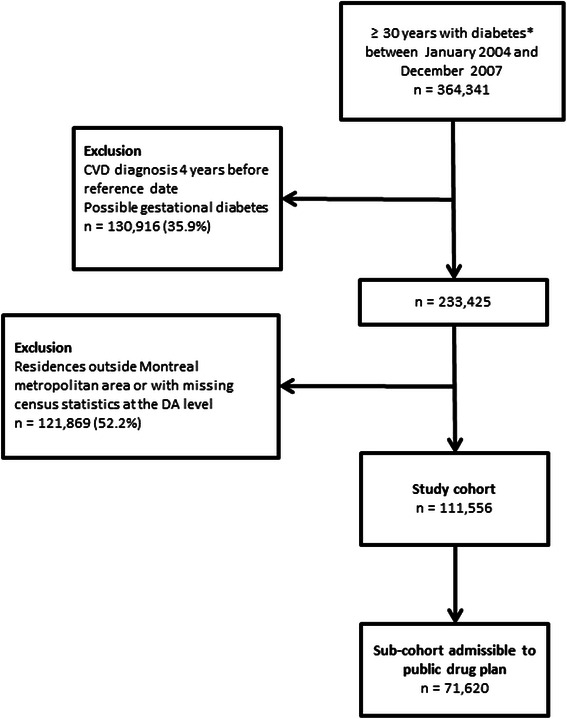
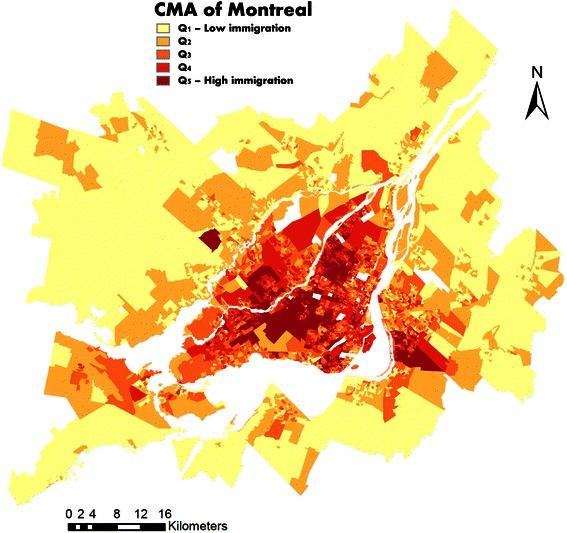
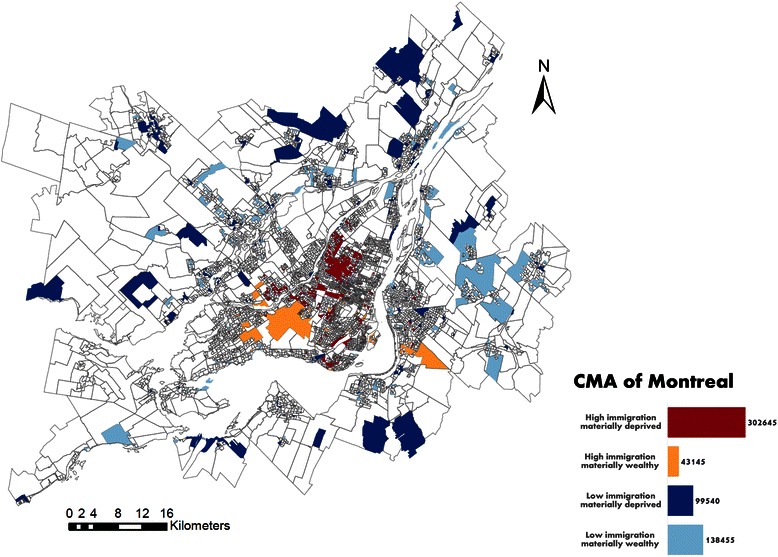
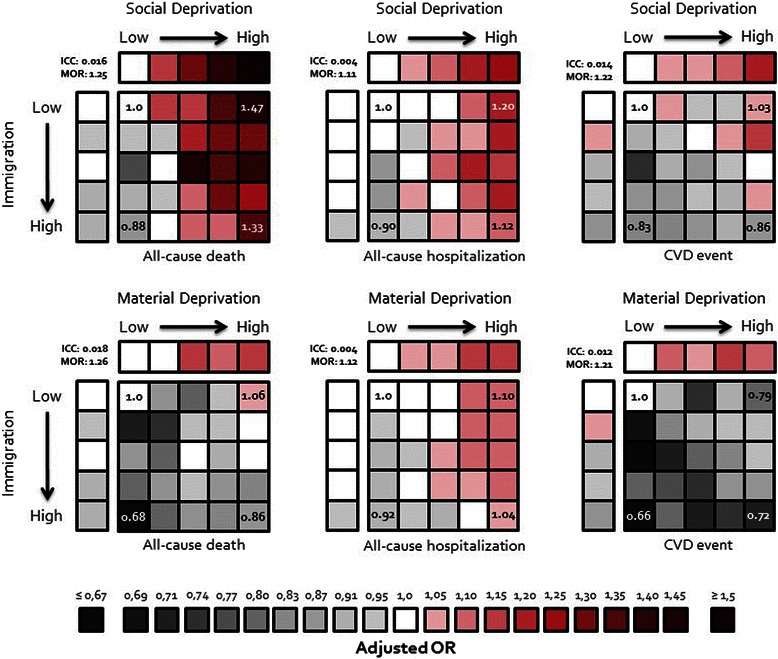
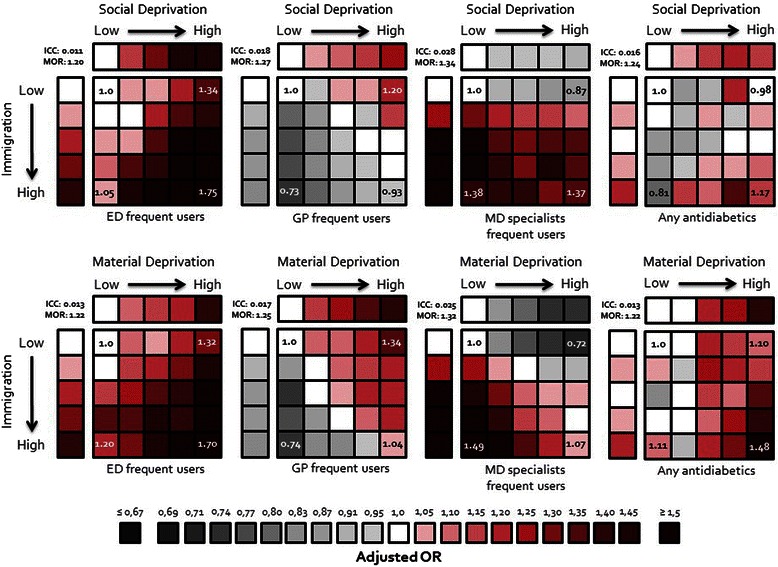
Methods: This is a secondary analysis of administrative data using a retrospective cohort of 111,556 patients living with diabetes without previous cardiovascular diseases (CVD) and living in the metropolitan region of Montreal (Canada). A score for immigration was calculated at the neighbourhood level using a principal component analysis with six neighbourhood-level variables (% of people with maternal language other than French or English, % of people who do not speak French or English, % of immigrants with different times since immigration (<5 years, 5-10 years, 10-15 years, 15-25 years)). Dependent variables were all-cause death, all-cause hospitalization, CVD event (death or hospitalization), frequent use of emergency departments, frequent use of general practitioner care, frequent use of specialist care, and purchase of at least one antidiabetic drug. For each of these variables, adjusted odds ratios were estimated using a multilevel logistic regression.
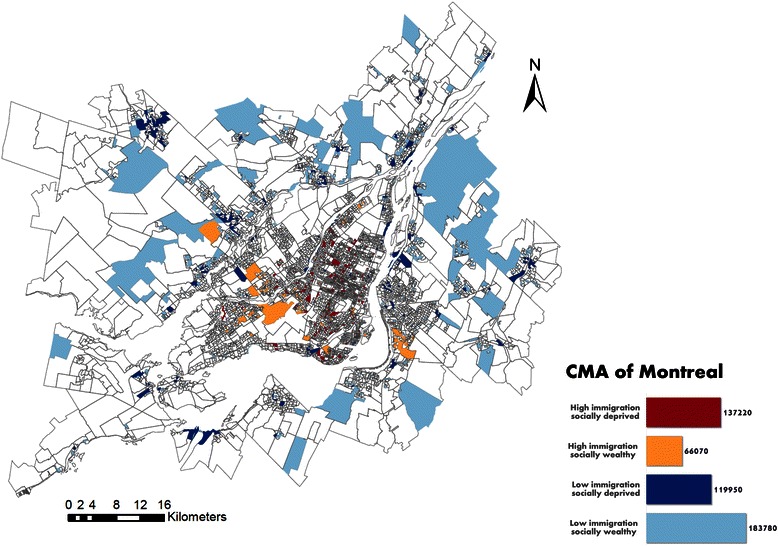
Results: Compared to patients with diabetes living in neighbourhoods with low immigration scores, those living in neighbourhoods with high immigration scores were less likely to die, to suffer a CVD event, to frequently visit general practitioners, but more likely to visit emergency departments or a specialist and to use an antidiabetic drug. These differences remained after controlling for patient-level variables such as age, sex, and comorbidities, as well as for neighbourhood attributes like material and social deprivation or living in the urban core.
Conclusions: In this study, patients with diabetes living in neighbourhoods with high immigration scores had different health outcomes and health care utilizations compared to those living in neighbourhoods with low immigration scores. Although we cannot disentangle the individual versus the area-based effect of immigration, these results may have an important impact for health care planning.
Figures
Similar articles
-
Factors associated with chronic frequent emergency department utilization in a population with diabetes living in metropolitan areas: a population-based retrospective cohort study.BMC Health Serv Res. 2017 Aug 4;17(1):525. doi: 10.1186/s12913-017-2453-3. BMC Health Serv Res. 2017. PMID: 28778161 Free PMC article.
-
Neighbourhood immigrant concentration and hospitalization: a multilevel analysis of cardiovascular-related admissions in Ontario using linked data.Can J Public Health. 2014 Sep 17;105(6):e404-11. doi: 10.17269/cjph.105.4616. Can J Public Health. 2014. PMID: 25560885 Free PMC article.
-
Neighbourhood deprivation and hospitalization for atrial fibrillation in Sweden.Europace. 2013 Aug;15(8):1119-27. doi: 10.1093/europace/eut019. Epub 2013 Feb 27. Europace. 2013. PMID: 23447572
-
Latino youth's internalising behaviours: links to immigrant status and neighbourhood characteristics.Ethn Health. 2013;18(3):315-35. doi: 10.1080/13557858.2012.734278. Epub 2012 Oct 31. Ethn Health. 2013. PMID: 23113641 Free PMC article. Review.
-
Immigration Status as the Foundational Determinant of Health for People Without Status in Canada: A Scoping Review.J Immigr Minor Health. 2022 Aug;24(4):1029-1044. doi: 10.1007/s10903-021-01273-w. Epub 2021 Oct 3. J Immigr Minor Health. 2022. PMID: 34601663 Free PMC article.
Cited by
-
Proximity and emergency department use: Multilevel analysis using administrative data from patients with cardiovascular risk factors.Can Fam Physician. 2015 Aug;61(8):e391-7. Can Fam Physician. 2015. PMID: 26505061 Free PMC article.
-
Neighbourhood socioeconomic status indices and early childhood development.SSM Popul Health. 2016 Nov 30;3:48-56. doi: 10.1016/j.ssmph.2016.11.006. eCollection 2017 Dec. SSM Popul Health. 2016. PMID: 29349203 Free PMC article.
-
Social and structural determinants of emergency department use among Arab and Jewish patients in Jerusalem.Int J Equity Health. 2022 Nov 7;21(1):156. doi: 10.1186/s12939-022-01698-1. Int J Equity Health. 2022. PMID: 36345031 Free PMC article.
-
Diabetes-related complications: Which research topics matter to diverse patients and caregivers?Health Expect. 2018 Apr;21(2):549-559. doi: 10.1111/hex.12649. Epub 2017 Nov 22. Health Expect. 2018. PMID: 29165920 Free PMC article.
-
Factors associated with chronic frequent emergency department utilization in a population with diabetes living in metropolitan areas: a population-based retrospective cohort study.BMC Health Serv Res. 2017 Aug 4;17(1):525. doi: 10.1186/s12913-017-2453-3. BMC Health Serv Res. 2017. PMID: 28778161 Free PMC article.
References
-
- Vanasse A, Courteau J, Lesage A, Fleury MJ, Grégoire JP, Moisan J, et al. Health inequities in mood disorders based on material and social deprivation in dwelling sectors. Can J Psychiatry. 2012;57(12):772–81. - PubMed
-
- Vanasse A, Courteau J, Asghari S, Leroux D, Cloutier L. Health inequalities associated with neighbourhood deprivation in the Quebec population with hypertension in primary prevention of cardiovascular disease. Chronic Dis Inj Can. 2014;34(4):181–94. - PubMed
-
- Statistics Canada. Immigration and Ethnocultural Diversity in Canada. Catalogue no. 99-010-X2011001. Available from: http://www12.statcan.gc.ca/nhs-enm/2011/as-sa/99-010-x/99-010-x2011001-e... (accessed January 2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
