

Thoracic epidural anesthesia improves outcomes in patients undergoing cardiac surgery: meta-analysis of randomized controlled trials
- PMID: 25888937
- PMCID: PMC4375848
- DOI: 10.1186/s40001-015-0091-y
Thoracic epidural anesthesia improves outcomes in patients undergoing cardiac surgery: meta-analysis of randomized controlled trials
Abstract
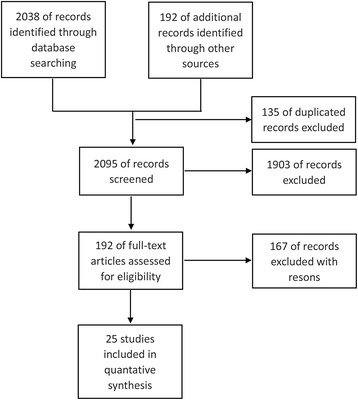
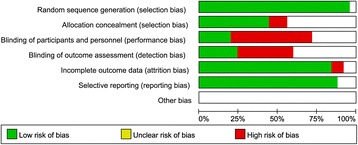
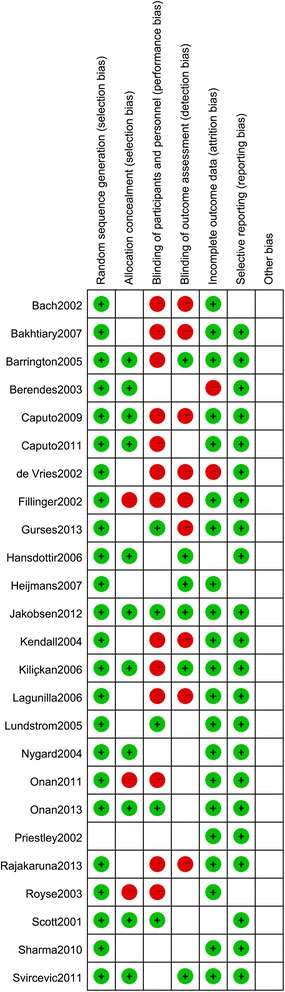
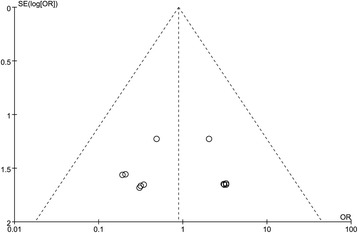
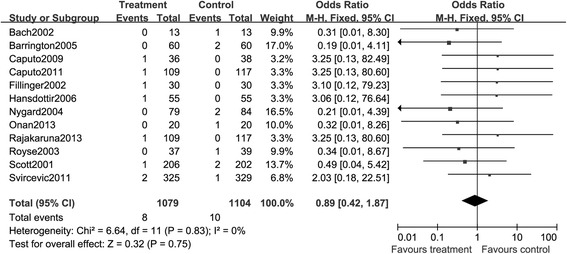
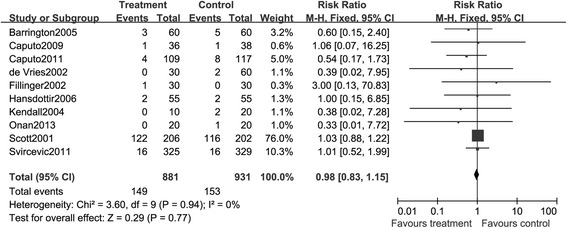
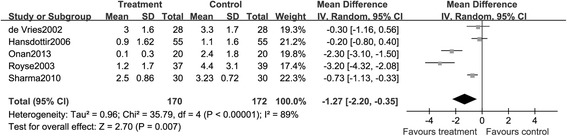
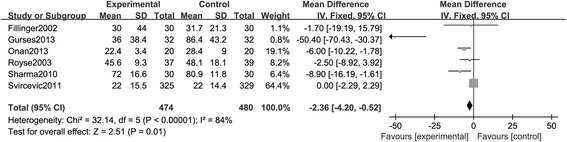
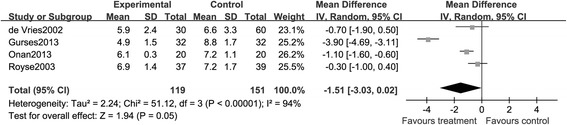
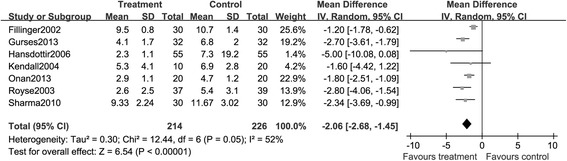
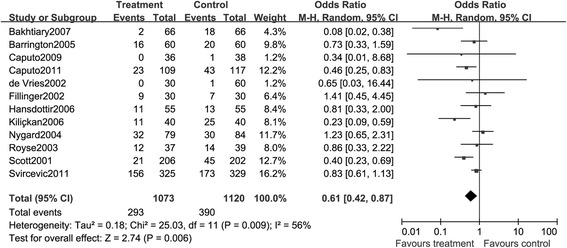
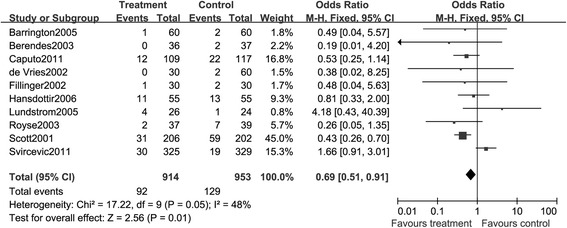
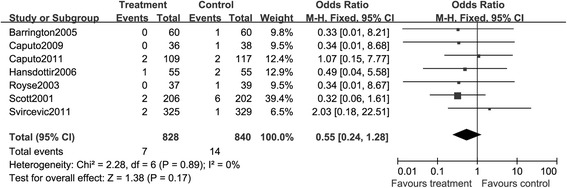
To assess the efficacy of thoracic epidural anesthesia (TEA) with or without general anesthesia (GA) versus GA in patients who underwent cardiac surgery, PubMed, Embase, the Cochrane online database, and Web of Science were searched with the limit of randomized controlled trials (RCTs) relevant to 'thoracic epidural anesthesia' and 'cardiac surgery'. Studies were identified and data were extracted by two reviewers independently. The quality of included studies was also assessed according to the Cochrane handbook. Outcomes of mortality, cardiac and respiratory functions, and treatment-associated complications were pooled and analyzed. The comprehensive search yielded 2,230 citations, and 25 of them enrolling 3,062 participants were included according to the inclusion criteria. Compared with GA alone, patients received TEA and GA showed reduced risks of death, myocardial infarction, and stroke, though there were no significant differences (P > 0.05). With regard to treatment-related complications, the pooled results for respiratory complications (risk ratio (RR), 0.69; 95% CI: 0.51, 0.91, P < 0.05), supraventricular arrhythmias (RR, 0.61; 95% CI: 0.42, 0.87, P < 0.05), and pain (mean difference (MD), -1.27; 95% CI: -2.20, -0.35, P < 0.05) were 0.69, 0.61, and -1.27, respectively. TEA was also associated with significant reduction of stays in intensive care unit (MD, -2.36; 95% CI: -4.20, -0.52, P < 0.05) and hospital (MD, -1.51; 95% CI: -3.03, 0.02, P > 0.05) and time to tracheal extubation (MD, -2.06; 95% CI:-2.68, -1.45, P < 0.05). TEA could reduce the risk of complications such as supraventricular arrhythmias, stays in hospital or intensive care unit, and time to tracheal extubation in patients who experienced cardiac surgery.
Figures
Similar articles
-
Meta-analysis of thoracic epidural anesthesia versus general anesthesia for cardiac surgery.Anesthesiology. 2011 Feb;114(2):271-82. doi: 10.1097/ALN.0b013e318201d300. Anesthesiology. 2011. PMID: 21239975 Review.
-
Thoracic Epidural Anesthesia in Cardiac Surgery: A Systematic Review, Meta-Analysis, and Trial Sequential Analysis of Randomized Controlled Trials.Anesth Analg. 2023 Sep 1;137(3):587-600. doi: 10.1213/ANE.0000000000006532. Epub 2023 May 23. Anesth Analg. 2023. PMID: 37220070
-
Comparison of three anesthetic techniques for off-pump coronary artery bypass grafting: general anesthesia, combined general and high thoracic epidural anesthesia, or high thoracic epidural anesthesia alone.J Cardiothorac Vasc Anesth. 2005 Feb;19(1):32-9. doi: 10.1053/j.jvca.2004.11.006. J Cardiothorac Vasc Anesth. 2005. PMID: 15747266 Clinical Trial.
-
Effects of perioperative central neuraxial analgesia on outcome after coronary artery bypass surgery: a meta-analysis.Anesthesiology. 2004 Jul;101(1):153-61. doi: 10.1097/00000542-200407000-00024. Anesthesiology. 2004. PMID: 15220785
-
Thoracic epidural anaesthesia for awake thoracic surgery in severely dyspnoeic patients excluded from general anaesthesia.Interact Cardiovasc Thorac Surg. 2014 Nov;19(5):816-23. doi: 10.1093/icvts/ivu230. Epub 2014 Jul 17. Interact Cardiovasc Thorac Surg. 2014. PMID: 25035439
Cited by
-
Pain management after robot-assisted minimally invasive esophagectomy.Heliyon. 2023 Feb 17;9(3):e13842. doi: 10.1016/j.heliyon.2023.e13842. eCollection 2023 Mar. Heliyon. 2023. PMID: 36895408 Free PMC article.
-
The effect of erector spinae plane block on arterial grafts in coronary artery bypass grafting.Turk Gogus Kalp Damar Cerrahisi Derg. 2023 Apr 28;31(2):186-191. doi: 10.5606/tgkdc.dergisi.2023.24089. eCollection 2023 Apr. Turk Gogus Kalp Damar Cerrahisi Derg. 2023. PMID: 37484629 Free PMC article.
-
Neuraxial Anesthesia and Analgesia During Cardiothoracic Surgery: A Narrative Review.Curr Pain Headache Rep. 2024 May;28(5):315-319. doi: 10.1007/s11916-024-01235-5. Epub 2024 Mar 20. Curr Pain Headache Rep. 2024. PMID: 38507134 Review.
-
Comparison of regional anesthetic techniques for postoperative analgesia after adult cardiac surgery: bayesian network meta-analysis.Front Cardiovasc Med. 2023 May 22;10:1078756. doi: 10.3389/fcvm.2023.1078756. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37283577 Free PMC article. Review.
-
Immediate extubation after cardiac surgery should be part of routine anesthesia practice for selected patients.Ann Card Anaesth. 2018 Apr-Jun;21(2):114-115. doi: 10.4103/aca.ACA_193_17. Ann Card Anaesth. 2018. PMID: 29652269 Free PMC article. No abstract available.
References
-
- Kirno K, Friberg P, Grzegorczyk A, Milocco I, Ricksten SE, Lundin S. Thoracic epidural anesthesia during coronary artery bypass surgery: effects on cardiac sympathetic activity, myocardial blood flow and metabolism, and central hemodynamics. Anesth Analg. 1994;79:1075–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
