

Clinical profile of Plasmodium falciparum and Plasmodium vivax infections in low and unstable malaria transmission settings of Colombia
- PMID: 25889074
- PMCID: PMC4397685
- DOI: 10.1186/s12936-015-0678-3
Clinical profile of Plasmodium falciparum and Plasmodium vivax infections in low and unstable malaria transmission settings of Colombia
Abstract
Background: Malaria transmission in Latin America is generally hypoendemic and unstable, with Plasmodium vivax as the most prevalent species. However, only a few studies have been carried out in areas with low and unstable transmission, whereas the clinical profile of malaria has been broadly described in hyperendemic areas. The pattern of clinical manifestations and laboratory findings in low to moderate endemic areas of Colombia is reported here.
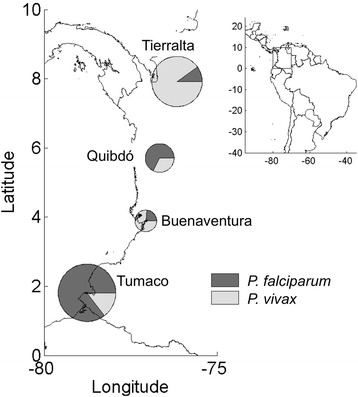
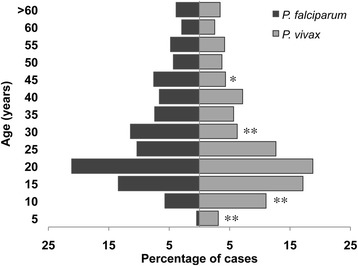
Methods: A passive surveillance study was conducted between 2011 and 2013 involving 1,328 patients with Plasmodium falciparum, P. vivax or mixed malaria infections attending malaria points-of-care of four malaria endemic-areas with distinct transmission intensities and parasite distribution. Trained physicians recorded clinical symptoms and signs as well as socio-demographic characteristics of study participants. Haematological, biochemical and urine tests were performed at the time of diagnosis.
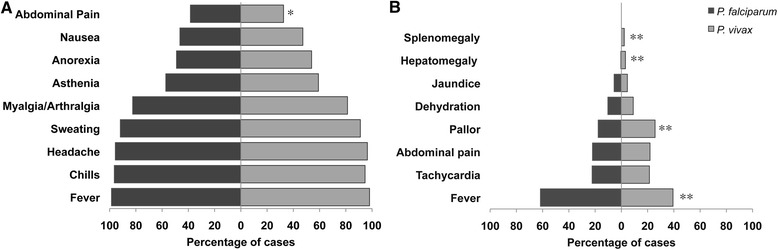
Results: Out of 1,328 cases, 673 (50.7%) were caused by P. vivax; 650 (48.9%) were due to P. falciparum; and five (0.4%) patients had mixed infections (P. falciparum/P. vivax). Most patients (92.5%) presented with uncomplicated malaria characterized by fever, chills, headache, sweating, myalgia/arthralgia and parasitaemia ≤ 20,000 parasites/μL. Fever, tachycardia, pallor and abdominal pain on palpation were more frequent in P. falciparum patients, whereas mild hepatomegaly and splenomegaly were mostly observed with P. vivax. Non-severe anaemia (Hb 7.0-10.9 g/dL) was observed in 20% of the subjects, whereas severe anaemia (Hb < 7.0 g/dL) was present in four patients. Half of the patients presented thrombocytopaenia regardless of parasite species. Leukopaenia, neutrophilia and monocytosis were frequently observed in patients infected with P. falciparum. Mild-to-moderate biochemical alterations were present in ~25% of the patients, particularly abnormal bilirubin in those with P. falciparum and abnormal transaminases in P. vivax malaria patients. Proteinuria was present in ~50% of the patients regardless of parasite species, whereas haemoglobinuria was more common in P. vivax infections. Only 7.5% of the cases were classified as clinically severe malaria, caused by both P. vivax and P. falciparum.
Conclusions: The high prevalence of uncomplicated malaria associated with moderate parasitaemia suggests the importance of timely diagnosis and effective treatment and encourages new activities to further decrease complicated malaria cases and mortality.
Figures
References
-
- WHO . World Malaria Report 2014. Geneva: World Health Organization; 2014. p. 227.
-
- Mendis K, Sina BJ, Marchesini P, Carter R. The neglected burden of Plasmodium vivax malaria. Am J Trop Med Hyg. 2001;64(1–2 Suppl):97–106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
