

CYP2B6*6, CYP2B6*18, Body weight and sex are predictors of efavirenz pharmacokinetics and treatment response: population pharmacokinetic modeling in an HIV/AIDS and TB cohort in Zimbabwe
- PMID: 25889207
- PMCID: PMC4405819
- DOI: 10.1186/s40360-015-0004-2
CYP2B6*6, CYP2B6*18, Body weight and sex are predictors of efavirenz pharmacokinetics and treatment response: population pharmacokinetic modeling in an HIV/AIDS and TB cohort in Zimbabwe
Abstract
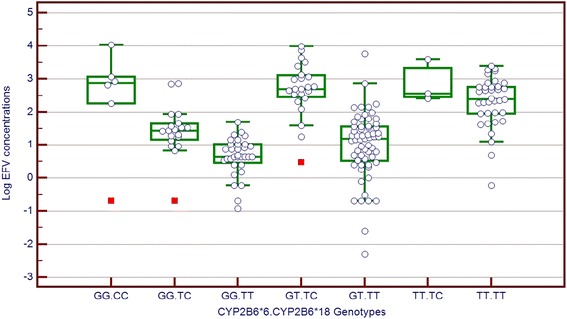
Background: Efavirenz (EFV) therapeutic response and toxicity are associated with high inter-individual variability attributed to variation in its pharmacokinetics. Plasma concentrations below 1 μg/ml may result in virologic failure and above 4 μg/ml, may result in central nervous system adverse effects. This study used population pharmacokinetics modeling to explore the influence of demographic and pharmacogenetic factors including efavirenz-rifampicin interaction on EFV pharmacokinetics, towards safer dosing of EFV.
Methods: Patients receiving an EFV-based regimen for their antiretroviral therapy and a rifampicin-containing anti-TB regimen were recruited. EFV plasma concentrations were measured by HPLC and genomic DNA genotyped for variants in the CYP2B6, CYP2A6 and ABCB1 genes. All patients were evaluated for central nervous system adverse effects characterised as sleep disorders, hallucinations and headaches using the WHO ADR grading system. A pharmacokinetic model was built in a forward and reverse procedure using nonlinear mixed effect modeling in NONMEM VI followed by model-based simulations for optimal doses.
Results: CYP2B6*6 and *18 variant alleles, weight and sex were the most significant covariates explaining 55% of inter-individual variability in EFV clearance. Patients with the CYP2B6*6TT genotype had a 63% decrease in EFV clearance despite their CYP2B6*18 genotypes with females having 22% higher clearance compared to males. There was a 21% increase in clearance for every 10 kg increase in weight. The effect of TB/HIV co-treatment versus HIV treatment only was not statistically significant. No clinically relevant association between CYP2B6 genotypes and CNS adverse effects was seen, but patients with CNS adverse effects had a 27% lower clearance compared to those without. Model- based simulations indicated that all carriers of CYP2B6*6 TT genotype would be recommended a dose reduction to 200 mg/day, while the majority of extensive metabolisers may be given 400 mg/day and still maintain therapeutic levels.
Conclusion: This study showed that screening for CYP2B6 functional variants has a high predictability for efavirenz plasma levels and could be used in prescribing optimal and safe EFV doses.
Figures

Similar articles
-
Genetic variants in CYP2B6 and CYP2A6 explain interindividual variation in efavirenz plasma concentrations of HIV-infected children with diverse ethnic origin.PLoS One. 2017 Sep 8;12(9):e0181316. doi: 10.1371/journal.pone.0181316. eCollection 2017. PLoS One. 2017. PMID: 28886044 Free PMC article.
-
The role of genetic polymorphisms in cytochrome P450 and effects of tuberculosis co-treatment on the predictive value of CYP2B6 SNPs and on efavirenz plasma levels in adult HIV patients.Antiviral Res. 2014 Feb;102:44-53. doi: 10.1016/j.antiviral.2013.11.011. Epub 2013 Dec 5. Antiviral Res. 2014. PMID: 24316028
-
Population Pharmacokinetic Model Linking Plasma and Peripheral Blood Mononuclear Cell Concentrations of Efavirenz and Its Metabolite, 8-Hydroxy-Efavirenz, in HIV Patients.Antimicrob Agents Chemother. 2017 Jul 25;61(8):e00207-17. doi: 10.1128/AAC.00207-17. Print 2017 Aug. Antimicrob Agents Chemother. 2017. PMID: 28559276 Free PMC article.
-
Pharmacokinetics of efavirenz in patients on antituberculosis treatment in high human immunodeficiency virus and tuberculosis burden countries: A systematic review.Br J Clin Pharmacol. 2018 Aug;84(8):1641-1658. doi: 10.1111/bcp.13600. Epub 2018 May 22. Br J Clin Pharmacol. 2018. PMID: 29624706 Free PMC article.
-
Role of Cytochrome P450 2B6 Pharmacogenomics in Determining Efavirenz-Mediated Central Nervous System Toxicity, Treatment Outcomes, and Dosage Adjustments in Patients with Human Immunodeficiency Virus Infection.Pharmacotherapy. 2016 Dec;36(12):1245-1254. doi: 10.1002/phar.1852. Epub 2016 Dec 4. Pharmacotherapy. 2016. PMID: 27779789 Review.
Cited by
-
CYP2B6 Functional Variability in Drug Metabolism and Exposure Across Populations-Implication for Drug Safety, Dosing, and Individualized Therapy.Front Genet. 2021 Jul 12;12:692234. doi: 10.3389/fgene.2021.692234. eCollection 2021. Front Genet. 2021. PMID: 34322158 Free PMC article. Review.
-
Population Pharmacokinetic-Pharmacogenetic (PopPK-PGx) Model of Efavirenz in HIV-1-Infected Patients.Cureus. 2025 Jul 22;17(7):e88533. doi: 10.7759/cureus.88533. eCollection 2025 Jul. Cureus. 2025. PMID: 40851704 Free PMC article.
-
Long-term efavirenz pharmacokinetics is comparable between Tanzanian HIV and HIV/Tuberculosis patients with the same CYP2B6*6 genotype.Sci Rep. 2018 Nov 5;8(1):16316. doi: 10.1038/s41598-018-34674-3. Sci Rep. 2018. PMID: 30397233 Free PMC article.
-
Impact of Population and Pharmacogenetics Variations on Efavirenz Pharmacokinetics and Immunologic Outcomes During Anti-Tuberculosis Co-Therapy: A Parallel Prospective Cohort Study in Two Sub-Sahara African Populations.Front Pharmacol. 2020 Feb 7;11:26. doi: 10.3389/fphar.2020.00026. eCollection 2020. Front Pharmacol. 2020. PMID: 32116703 Free PMC article.
-
A review of clinical pharmacogenetics Studies in African populations.Per Med. 2020 Mar;17(2):155-170. doi: 10.2217/pme-2019-0110. Epub 2020 Mar 3. Per Med. 2020. PMID: 32125935 Free PMC article. Review.
References
-
- Guidelines for Antiretroviral Therapy in Zimbabwe. The National Drug and Therapeutics Policy Advisory Committee (NDTPAC) and The AIDS and TB Unit, Ministry of Health and Child Welfare (MOHCW), Harare, Republic of Zimbabwe. 2010
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
