

Intensity-modulated Total Body Irradiation (TBI) with TomoDirect™
- PMID: 25889227
- PMCID: PMC4353674
- DOI: 10.1186/s13014-015-0362-3
Intensity-modulated Total Body Irradiation (TBI) with TomoDirect™
Abstract
Background: The new TomoDirect™ modality offers a non-rotational option with discrete beam angles. We have investigated this mode for TBI with the intention to test the feasibility and to establish it as a clinical routine method. Special foci were directed onto treatment planning, dosimetric accuracy and practical aspects.
Patients and methods: TBI plans were calculated with TomoDirect™ for a Rando™ phantom and all patients with an intended fractionated total body irradiation between November 2013 and May 2014 (n = 8). Finally, four of these patients were irradiated with TomoDirect™. Additionally we studied variations in the modulation factor, pitch, field width of Y-jaws and dose grid during optimization. Dose measurements were performed using thermoluminescent rods in the Rando™ phantom, with the Delta4® and with ionization chambers in a solid water phantom.
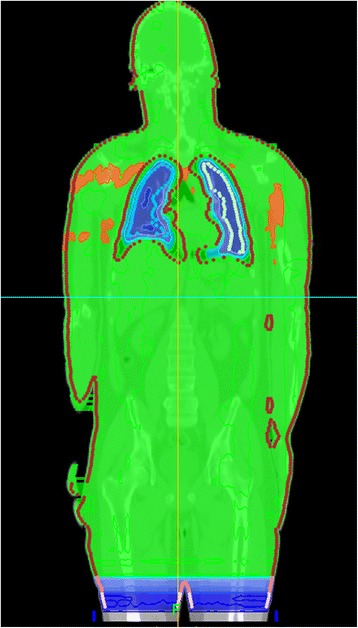
Results: For all eight calculated plans with a prescribed dose of 12 Gy Dmean was 12.09-12.33 Gy (12,25 ± 0.08 Gy), D98 11.2-11.6 Gy (11.45 ± 0.12 Gy) and D2 12.6-13.1 Gy (12.94 ± 0.13 Gy). Dmean of inner lungs was 8.73 ± 0.22 Gy on the left side and 8.69 ± 0.27 Gy on the right side. When single planning parameters are varied with otherwise constant parameters, the modulation factor showed the greatest impact on dose homogeneity and treatment time. The impact of the pitch was marginally, and almost equal homogeneity can be obtained with field width of Y-jaws 5 cm and 2.5 cm. Measurements with thermoluminescent rods (n = 25) in the Rando™ phantom showed a mean dose deviation between measured and calculated dose of 0.66 ± 2.26%. 18 of 25 TLDs had a deviation below 3%, seven of 25 TLDs between 3% and 5%.
Conclusion: TBI with TomoDirect™ allows a superior homogeneity compared to conventional methods, where lung blocks are widely accepted. The treatment is performed only in supine position and is robust and comfortable for the patient. TomoDirect™ allows the implementation of organ-specific dose prescriptions. So the discussion about the balance between the need for aggressive treatment and limited toxicity can be renewed with the new potentials of TomoDirect™ - for children as well as for adults - and possibly yield a better clinical outcome in the future.
Figures




References
-
- Sanchez-Doblado F, Quast U, Arrans R, Errazquin L, Sanchez-Nieto B, Terron JA. Total body irradiation prior to bone marrow transplantation. Report of European Group for Blood and Marrow Transplantation. Sevilla; 1995.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
