

Clinical features of subclinical left ventricular systolic dysfunction in patients with diabetes mellitus
- PMID: 25889250
- PMCID: PMC4404084
- DOI: 10.1186/s12933-015-0201-8
Clinical features of subclinical left ventricular systolic dysfunction in patients with diabetes mellitus
Abstract
Background: Left ventricular (LV) longitudinal systolic dysfunction has been identified even in asymptomatic patients with diabetes mellitus (DM) and preserved LV ejection fraction (LVEF). However, its relevant clinical features have not been fully evaluated.
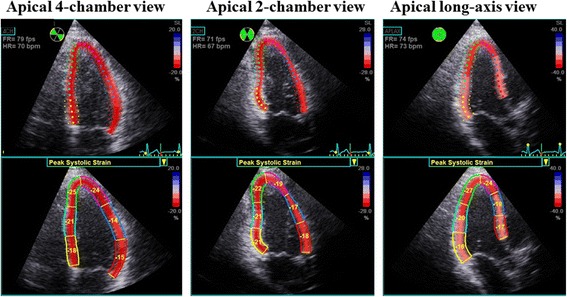
Methods: We studied 144 asymptomatic DM patients without coronary artery disease. Their mean age was 57 ± 15 years, 79 (55%) were female, and mean LVEF was 66 ± 4% (all ≥50%). Global longitudinal strain (GLS) was determined as the average peak strain of 18 segments from the three standard apical views, and was expressed as an absolute value. With the pre-defined cutoff for subclinical LV systolic dysfunction in DM patients with preserved LVEF set at GLS < 18%, this dysfunction was detected in 53 patients (37%).
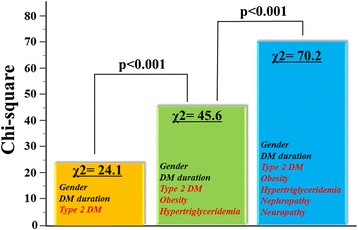
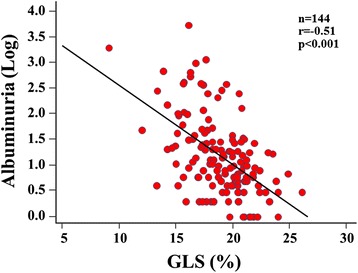
Results: Multivariate logistic regression analysis revealed that type 2 DM, hypertriglyceridemia, overweight/obesity, nephropathy and neuropathy were independently associated with GLS < 18%, with nephropathy being the highest risk factor (OR: 5.26; 95% CI 2.111-13.12, p < 0.001). For sequential logistic regression models, a model based on clinical variables including gender, type 2 DM and DM duration (χ(2) = 24.1) was improved by addition of overweight/obesity and hypertriglyceridemia (χ(2) = 45.6, p < 0.001), and further improved by addition of nephropathy and neuropathy (χ(2) = 70.2, p < 0.001) as variables. Furthermore, albuminuria significantly correlated with GLS (r = -0.51, p < 0.001), and a multivariate regression model showed it to be the factor most closely associated with GLS (β = -0.33, p < 0.001).
Conclusions: Diabetic complications, hypertriglyceridemia and overweight/obesity were closely associated with early stage of LV systolic longitudinal myocardial dysfunction in asymptomatic DM patients with preserved LVEF. Our findings can be clinically noticeable for the management of DM patients.
Figures
References
-
- Ryden L, Grant PJ, Anker SD, Berne C, Cosentino F, Danchin N, et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD) Eur Heart J. 2013;34(39):3035–87. doi: 10.1093/eurheartj/eht108. - DOI - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–239. doi: 10.1016/j.jacc.2013.05.019. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
