

The potential impact of moxidectin on onchocerciasis elimination in Africa: an economic evaluation based on the Phase II clinical trial data
- PMID: 25889256
- PMCID: PMC4381491
- DOI: 10.1186/s13071-015-0779-4
The potential impact of moxidectin on onchocerciasis elimination in Africa: an economic evaluation based on the Phase II clinical trial data
Abstract
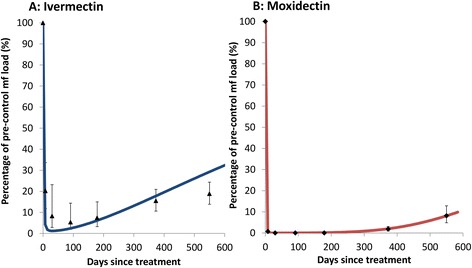
Background: Spurred by success in several foci, onchocerciasis control policy in Africa has shifted from morbidity control to elimination of infection. Clinical trials have demonstrated that moxidectin is substantially more efficacious than ivermectin in effecting sustained reductions in skin microfilarial load and, therefore, may accelerate progress towards elimination. We compare the potential cost-effectiveness of annual moxidectin with annual and biannual ivermectin treatment.
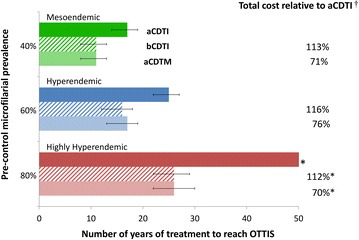
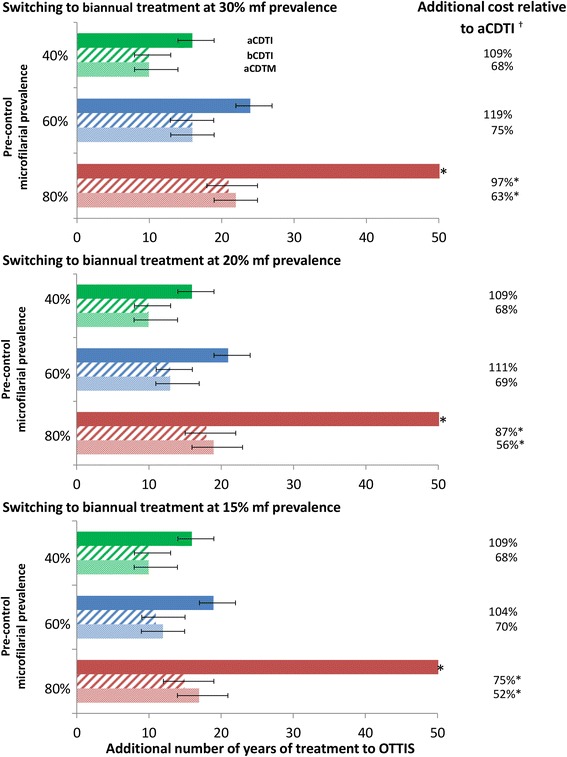
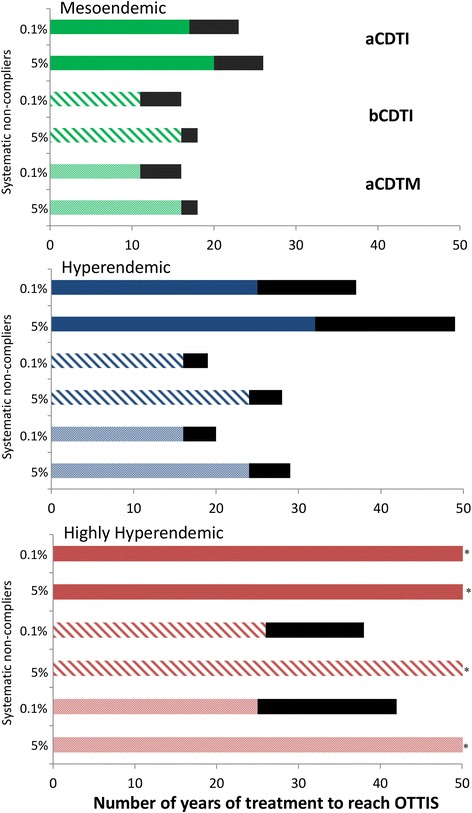
Methods: Data from the first clinical study of moxidectin were used to parameterise the onchocerciasis transmission model EPIONCHO to investigate, for different epidemiological and programmatic scenarios in African savannah settings, the number of years and in-country costs necessary to reach the operational thresholds for cessation of treatment, comparing annual and biannual ivermectin with annual moxidectin treatment.
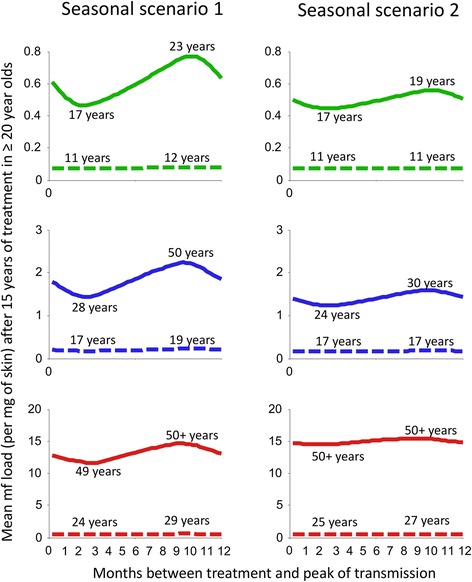
Results: Annual moxidectin and biannual ivermectin treatment would achieve similar reductions in programme duration relative to annual ivermectin treatment. Unlike biannual ivermectin treatment, annual moxidectin treatment would not incur a considerable increase in programmatic costs and, therefore, would generate sizeable in-country cost savings (assuming the drug is donated). Furthermore, the impact of moxidectin, unlike ivermectin, was not substantively influenced by the timing of treatment relative to seasonal patterns of transmission.
Conclusions: Moxidectin is a promising new drug for the control and elimination of onchocerciasis. It has high programmatic value particularly when resource limitation prevents a biannual treatment strategy, or optimal timing of treatment relative to peak transmission season is not feasible.
Figures
Similar articles
-
Reaching the london declaration on neglected tropical diseases goals for onchocerciasis: an economic evaluation of increasing the frequency of ivermectin treatment in Africa.Clin Infect Dis. 2014 Oct;59(7):923-32. doi: 10.1093/cid/ciu467. Epub 2014 Jun 18. Clin Infect Dis. 2014. PMID: 24944228 Free PMC article.
-
An Updated Economic Assessment of Moxidectin Treatment Strategies for Onchocerciasis Elimination.Clin Infect Dis. 2024 Apr 25;78(Suppl 2):S138-S145. doi: 10.1093/cid/ciae054. Clin Infect Dis. 2024. PMID: 38662693 Free PMC article.
-
Moxidectin: an oral treatment for human onchocerciasis.Expert Rev Anti Infect Ther. 2020 Nov;18(11):1067-1081. doi: 10.1080/14787210.2020.1792772. Epub 2020 Jul 26. Expert Rev Anti Infect Ther. 2020. PMID: 32715787 Review.
-
Can mass drug administration of moxidectin accelerate onchocerciasis elimination in Africa?Philos Trans R Soc Lond B Biol Sci. 2023 Oct 9;378(1887):20220277. doi: 10.1098/rstb.2022.0277. Epub 2023 Aug 21. Philos Trans R Soc Lond B Biol Sci. 2023. PMID: 37598705 Free PMC article.
-
Onchodermatitis.Curr Opin Infect Dis. 2010 Apr;23(2):124-31. doi: 10.1097/QCO.0b013e328336a256. Curr Opin Infect Dis. 2010. PMID: 20071985 Review.
Cited by
-
Efficacy and Safety of Moxidectin, Synriam, Synriam-Praziquantel versus Praziquantel against Schistosoma haematobium and S. mansoni Infections: A Randomized, Exploratory Phase 2 Trial.PLoS Negl Trop Dis. 2016 Sep 16;10(9):e0005008. doi: 10.1371/journal.pntd.0005008. eCollection 2016 Sep. PLoS Negl Trop Dis. 2016. PMID: 27636542 Free PMC article. Clinical Trial.
-
Onchodermatitis: Where Are We Now?Trop Med Infect Dis. 2018 Sep 1;3(3):94. doi: 10.3390/tropicalmed3030094. Trop Med Infect Dis. 2018. PMID: 30274490 Free PMC article. Review.
-
Current perspective of new anti-Wolbachial and direct-acting macrofilaricidal drugs as treatment strategies for human filariasis.GMS Infect Dis. 2022 Mar 30;10:Doc02. doi: 10.3205/id000079. eCollection 2022. GMS Infect Dis. 2022. PMID: 35463816 Free PMC article. Review.
-
Required duration of mass ivermectin treatment for onchocerciasis elimination in Africa: a comparative modelling analysis.Parasit Vectors. 2015 Oct 22;8:552. doi: 10.1186/s13071-015-1159-9. Parasit Vectors. 2015. PMID: 26489937 Free PMC article.
-
Why onchocerciasis transmission persists after 15 annual ivermectin mass drug administrations in South-West Cameroon.BMJ Glob Health. 2021 Jan;6(1):e003248. doi: 10.1136/bmjgh-2020-003248. BMJ Glob Health. 2021. PMID: 33431378 Free PMC article.
References
-
- World Health Organization. 18th Session of the Joint Action Forum. Bujumbura, Burundi; 2012. http://www.who.int/apoc/media/Journal_du_FAC_day_4_Anglais.pdf
-
- London Declaration on Neglected Tropical Diseases. Ending the neglect and reaching 2020 goals. London, UK; 2012. http://unitingtocombatntds.org/downloads/press/ntd_event_london_declarat...
-
- World Health Organization Progress towards eliminating onchocerciasis in the WHO Region of the Americas: verification by WHO of elimination of transmission in Colombia. Wkly Epidemiol Rec. 2013;88(36):381–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
