

Anti-inflammatory and morphologic effects of pitavastatin on carotid arteries and thoracic aorta evaluated by integrated backscatter trans-esophageal ultrasound and PET/CT: a prospective randomized comparative study with pravastatin (EPICENTRE study)
- PMID: 25889304
- PMCID: PMC4387666
- DOI: 10.1186/s12947-015-0012-9
Anti-inflammatory and morphologic effects of pitavastatin on carotid arteries and thoracic aorta evaluated by integrated backscatter trans-esophageal ultrasound and PET/CT: a prospective randomized comparative study with pravastatin (EPICENTRE study)
Abstract
Background: We sought to evaluate the effects of a strong lipophilic statin (pitavastatin) on plaque components and morphology assessed by transesophageal echocardiography (TEE) and transthoracic echocardiography (TTE), as well as plaque inflammation assessed by 18F-fluorodeoxyglucose (FDG) PET/CT in the thoracic aorta and the carotid artery. Furthermore, we compared the effects of pitavastatin with those of mild hydrophilic statin (pravastatin).
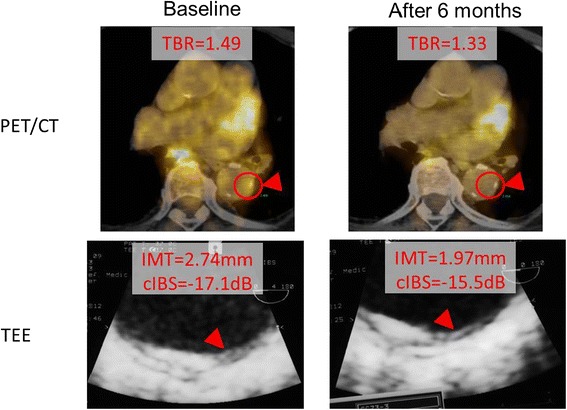
Methods: We examined atherosclerotic plaques in the thoracic aorta by TEE and those in the carotid artery by integrated backscatter (IBS)-TTE and PET/CT. We identified the target plaque, where there was macrophage infiltration and inflammation, by strong FDG uptake in the thoracic aorta and carotid arteries and measured maximum standard uptake values (max SUV) by PET/CT. We measured the intima-media thickness (IMT) and the corrected IBS (cIBS) values in the intima-media complex by TEE and TTE at the same site of FDG accumulation by PET/CT.
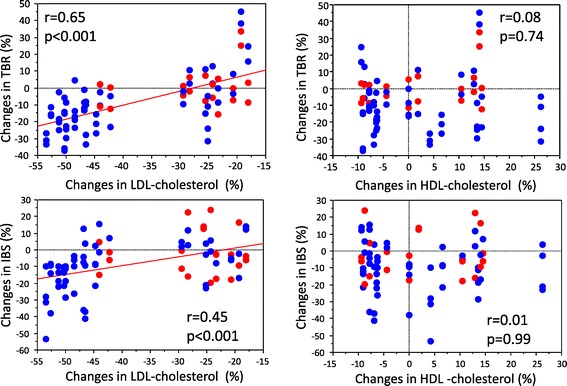
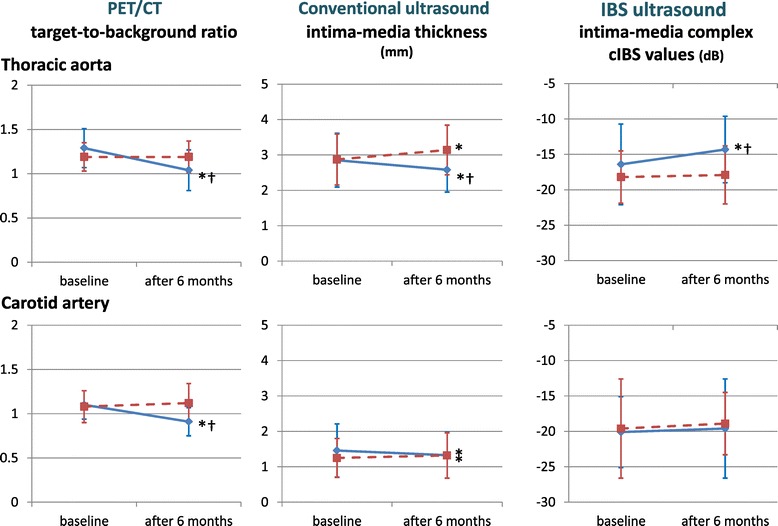
Results: Patients were randomly divided into two treatment groups: a pitavastatin group (PI group: n =10, 68.4 ± 5.1 years) and a pravastatin group (PR group: n =10, 63.9 ± 11.2 years). The same examinations were performed after six months at the same site in each patient. We used calculated target-to-background ratio (TBR) to measure max SUV of plaques and evaluated percent change of TBR. There was no significant difference in low density lipoprotein-cholesterol, TBR, IMT and cIBS values in plaques at baseline between the PI and PR groups. After treatment, there was greater improvement in TBR, cIBS values and IMT in the PI group than the PR group.
Conclusions: The pravastatin treatment was less effective on plaque inflammation than pitavastatin treatment. This trend was the same in the carotid arteries and the thoracic aorta. Pitavastatin not only improved the atherosis as measured by IMT and cIBS values but also attenuated inflammation of plaques as measured by max SUV at the same site. The present study indicated that pitavastatin has stronger effects on the regression and stabilization of plaques in the thoracic aorta and carotid arteries compared with pravastatin.
Figures
Similar articles
-
Integrated backscatter and intima-media thickness of the thoracic aorta evaluated by transesophageal echocardiography in hypercholesterolemic patients: effect of pitavastatin therapy.Ultrasound Med Biol. 2009 Feb;35(2):193-200. doi: 10.1016/j.ultrasmedbio.2008.08.011. Epub 2008 Oct 31. Ultrasound Med Biol. 2009. PMID: 18977068 Clinical Trial.
-
Higher reliability of 18F-FDG target background ratio compared to standardized uptake value in vulnerable carotid plaque detection: a pilot study.Ann Nucl Med. 2014 Jul;28(6):571-9. doi: 10.1007/s12149-014-0850-9. Epub 2014 Apr 16. Ann Nucl Med. 2014. PMID: 24737136
-
18F-FDG accumulation in atherosclerosis: use of CT and MR co-registration of thoracic and carotid arteries.Eur J Nucl Med Mol Imaging. 2006 May;33(5):589-94. doi: 10.1007/s00259-005-0005-2. Epub 2006 Feb 21. Eur J Nucl Med Mol Imaging. 2006. PMID: 16491424 Clinical Trial.
-
Variability and uncertainty of 18F-FDG PET imaging protocols for assessing inflammation in atherosclerosis: suggestions for improvement.J Nucl Med. 2015 Apr;56(4):552-9. doi: 10.2967/jnumed.114.142596. Epub 2015 Feb 26. J Nucl Med. 2015. PMID: 25722452 Review.
-
FDG PET/CT Imaging of Carotid Atherosclerosis.Neuroimaging Clin N Am. 2016 Feb;26(1):45-54. doi: 10.1016/j.nic.2015.09.004. Neuroimaging Clin N Am. 2016. PMID: 26610659 Review.
Cited by
-
Noninvasive Molecular Imaging of Disease Activity in Atherosclerosis.Circ Res. 2016 Jul 8;119(2):330-40. doi: 10.1161/CIRCRESAHA.116.307971. Circ Res. 2016. PMID: 27390335 Free PMC article. Review.
-
Effect of statins on arterial wall inflammation as assessed by 18F-FDG PET CT: an updated systematic review and meta-analysis.J Inflamm (Lond). 2024 Dec 18;21(1):52. doi: 10.1186/s12950-024-00421-x. J Inflamm (Lond). 2024. PMID: 39696570 Free PMC article.
-
Carotid plaque inflammatory activity assessed by 2-[18F]FDG-PET imaging decrease after a neurological thromboembolic event.EJNMMI Res. 2021 Mar 23;11(1):30. doi: 10.1186/s13550-021-00773-y. EJNMMI Res. 2021. PMID: 33755791 Free PMC article.
-
Effect of Statin Therapy on Arterial Wall Inflammation Based on 18F-FDG PET/CT: A Systematic Review and Meta-Analysis of Interventional Studies.J Clin Med. 2019 Jan 18;8(1):118. doi: 10.3390/jcm8010118. J Clin Med. 2019. PMID: 30669380 Free PMC article. Review.
-
Carotid Artery Temperature Reduction with Statin Therapy in Patients with Familial Hyperlipidemia Syndromes.J Clin Med. 2021 Oct 27;10(21):5008. doi: 10.3390/jcm10215008. J Clin Med. 2021. PMID: 34768528 Free PMC article.
References
-
- Taylor AJ, Kent SM, Flaherty PJ, Coyle LC, Markwood TT, Vernalis MN. ARBITER: Arterial biology for the investigation of the treatment effects of reducing cholesterol. A randomized trial comparing the effects of atorvastatin and pravastatin on carotid intima medial thickness. Circulation. 2002;106:2055–60. doi: 10.1161/01.CIR.0000034508.55617.65. - DOI - PubMed
-
- Long-Term Investigation with Pravastatin in Ischemic Disease (LIPID) Study Group Prevention of cardiovascular events and death with pravastatin in patient with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–57. doi: 10.1056/NEJM199811053391902. - DOI - PubMed
-
- Kawasaki M, Ito Y, Yokoyama H, Arai M, Takemura G, Hara A, et al. Assessment of arterial medial characteristics in human carotid arteries using integrated backscatter ultrasound and its histological implications. Atherosclerosis. 2005;180:145–54. doi: 10.1016/j.atherosclerosis.2004.11.018. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
