

Xanthine oxidase inhibition alleviates the cardiac complications of insulin resistance: effect on low grade inflammation and the angiotensin system
- PMID: 25889404
- PMCID: PMC4355989
- DOI: 10.1186/s12967-015-0445-9
Xanthine oxidase inhibition alleviates the cardiac complications of insulin resistance: effect on low grade inflammation and the angiotensin system
Abstract
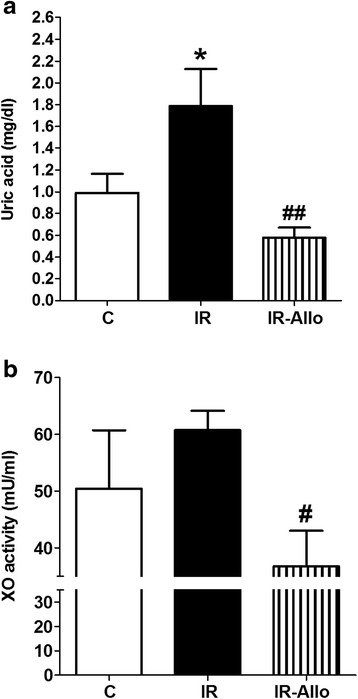
Background: We have previously shown that hyperuricemia plays an important role in the vascular complications of insulin resistance (IR). Here we investigated the effect of xanthine oxidase (XO) inhibition on the cardiac complications of IR.
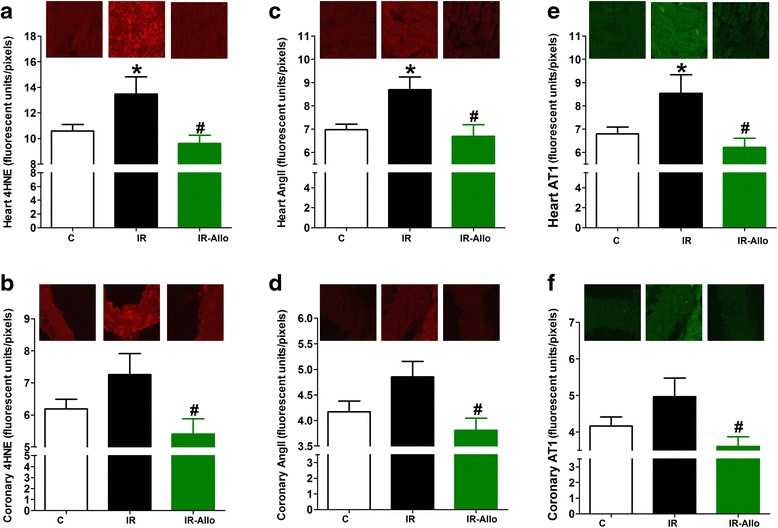
Methods: IR was induced in rats by a high fructose high fat diet for 12 weeks. Allopurinol, a standard XO inhibitor, was administered in the last 4 weeks before cardiac hemodynamics and electrocardiography, serum glucose, insulin, tumor necrosis factor alpha (TNFα), 8-isoprostane, uric acid, lactate dehydrogenase (LDH) and XO activity were measured. Expression of cardiac angiotensin II (AngII) and angiotensin receptor 1 (AT1) were assessed by immunofluorescence.
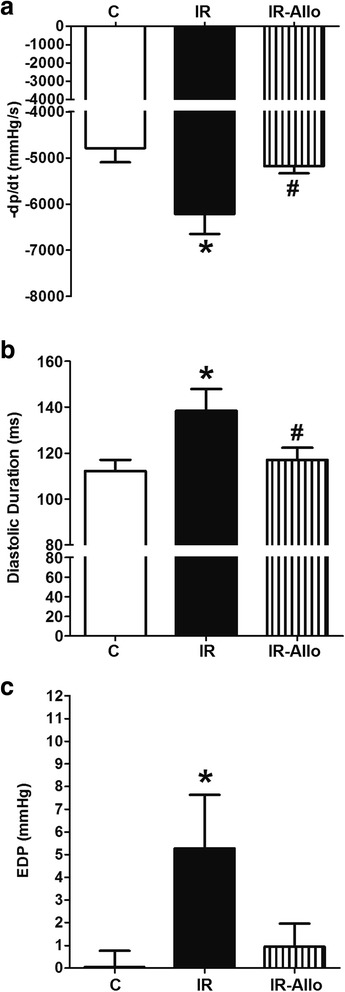
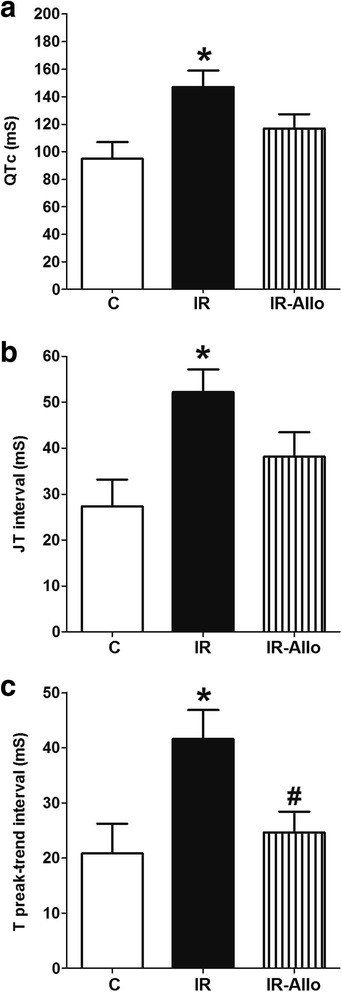
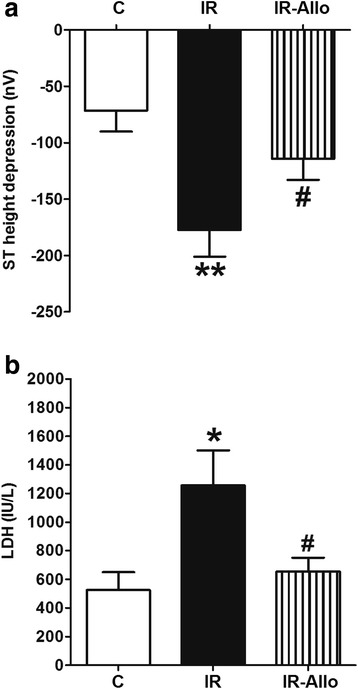
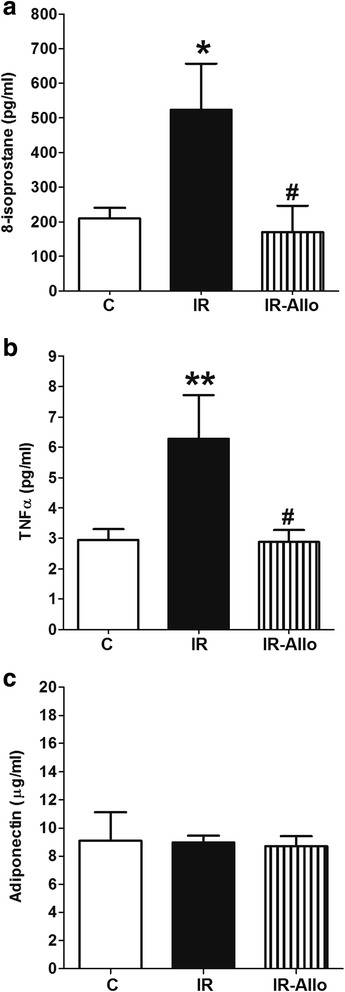
Results: IR animals had significant hyperuricemia which was inhibited by allopurinol administration. IR was associated with impaired ventricular relaxation (reflected by a decreased diastolic pressure increment and prolonged diastolic duration) and XO inhibition greatly attenuated impaired relaxation. IR was accompanied by cardiac ischemia (reflected by increased QTc and T peak trend intervals) while XO inhibition alleviated the ECG abnormalities. When subjected to isoproterenol-induced ischemia, IR hearts were less resistant (reflected by larger ST height depression and higher LDH level) while XO inhibition alleviated the accompanying ischemia. In addition, XO inhibition prevented the elevation of serum 8-isoprostane and TNFα, and blocked elevated AngII and AT1 receptor expression in the heart tissue of IR animals. However, XO inhibition did not affect the developed hyperinsulinemia or dyslipidemia.
Conclusions: XO inhibition alleviates cardiac ischemia and impaired relaxation in IR through the inhibition of low grade inflammation and the angiotensin system.
Figures
Similar articles
-
Preconditioning protects endothelium by preventing ET-1-induced activation of NADPH oxidase and xanthine oxidase in post-ischemic heart.J Mol Cell Cardiol. 2007 Feb;42(2):400-10. doi: 10.1016/j.yjmcc.2006.10.014. Epub 2006 Dec 6. J Mol Cell Cardiol. 2007. PMID: 17156794
-
Pentoxifylline alleviates cardiac ischemia and dysfunction following experimental angina in insulin resistance.PLoS One. 2014 May 29;9(5):e98281. doi: 10.1371/journal.pone.0098281. eCollection 2014. PLoS One. 2014. PMID: 24874295 Free PMC article.
-
Xanthine oxidase inhibition protects against Western diet-induced aortic stiffness and impaired vasorelaxation in female mice.Am J Physiol Regul Integr Comp Physiol. 2017 Aug 1;313(2):R67-R77. doi: 10.1152/ajpregu.00483.2016. Epub 2017 May 24. Am J Physiol Regul Integr Comp Physiol. 2017. PMID: 28539355 Free PMC article.
-
Allopurinol, xanthine oxidase, and cardiac ischemia.J Investig Med. 2009 Dec;57(8):902-9. doi: 10.2310/JIM.0b013e3181bca50c. J Investig Med. 2009. PMID: 19794315 Review.
-
Uric acid, heart failure survival, and the impact of xanthine oxidase inhibition.Congest Heart Fail. 2012 May-Jun;18(3):179-82. doi: 10.1111/j.1751-7133.2011.00262.x. Epub 2011 Nov 9. Congest Heart Fail. 2012. PMID: 22587748 Review.
Cited by
-
Pterostilbene Attenuates Fructose-Induced Myocardial Fibrosis by Inhibiting ROS-Driven Pitx2c/miR-15b Pathway.Oxid Med Cell Longev. 2019 Dec 4;2019:1243215. doi: 10.1155/2019/1243215. eCollection 2019. Oxid Med Cell Longev. 2019. PMID: 31871537 Free PMC article.
-
Assessment of the relationship between serum xanthine oxidase levels and type 2 diabetes: a cross-sectional study.Sci Rep. 2022 Dec 2;12(1):20816. doi: 10.1038/s41598-022-25413-w. Sci Rep. 2022. PMID: 36460780 Free PMC article.
-
Hydrogen sulfide stimulates xanthine oxidoreductase conversion to nitrite reductase and formation of NO.Redox Biol. 2020 Jul;34:101447. doi: 10.1016/j.redox.2020.101447. Epub 2020 Jan 30. Redox Biol. 2020. PMID: 32035920 Free PMC article.
-
Uric acid and transforming growth factor in fructose-induced production of reactive oxygen species in skeletal muscle.Nutr Rev. 2016 Apr;74(4):259-66. doi: 10.1093/nutrit/nuv111. Epub 2016 Mar 5. Nutr Rev. 2016. PMID: 26946251 Free PMC article. Review.
-
Self-Nanoemulsifying Drug Delivery System Loaded with Psiadia punctulata Major Metabolites for Hypertensive Emergencies: Effect on Hemodynamics and Cardiac Conductance.Front Pharmacol. 2021 Jun 10;12:681070. doi: 10.3389/fphar.2021.681070. eCollection 2021. Front Pharmacol. 2021. PMID: 34177590 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
