

Recommendations for malaria prevention in moderate to low risk areas: travellers' choice and risk perception
- PMID: 25889529
- PMCID: PMC4396190
- DOI: 10.1186/s12936-015-0654-y
Recommendations for malaria prevention in moderate to low risk areas: travellers' choice and risk perception
Abstract
Background: The considerable malaria decline in several countries challenges the strategy of chemoprophylaxis for travellers visiting moderate- to low-risk areas. An international consensus on the best strategy is lacking. It is essential to include travellers' opinions in the decision process. The preference of travellers regarding malaria prevention for moderate- to low-risk areas, related to their risk perception, as well as the reasons for their choices were investigated.
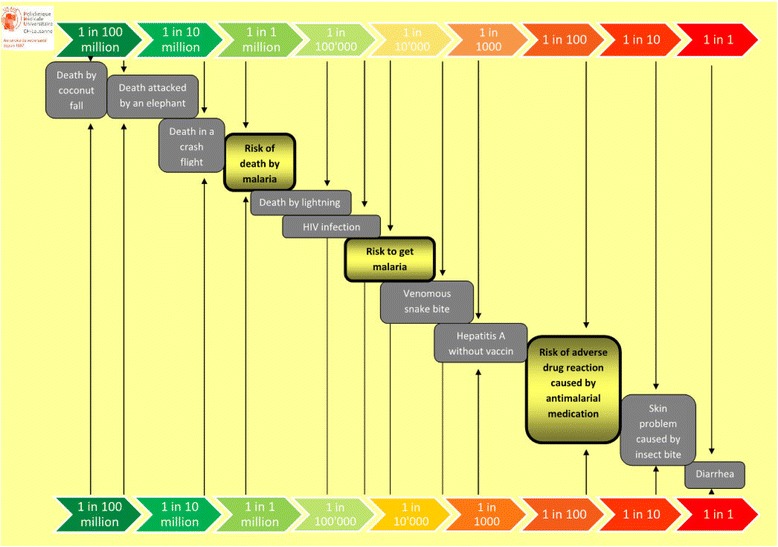
Methods: Prior to pre-travel consultation in the Travel Clinic, a self-administered questionnaire was given to travellers visiting moderate- to low-risk malaria areas. Four preventive options were proposed to the traveller, i.e., bite prevention only, chemoprophylaxis, stand-by emergency treatment alone, and stand-by emergency treatment with rapid diagnostic test. The information was accompanied by a risk scale for incidence of malaria, anti-malarial adverse drug reactions and other travel-related risks, inspired by Paling palettes from the Risk Communication Institute.
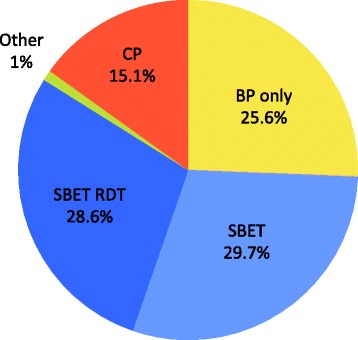
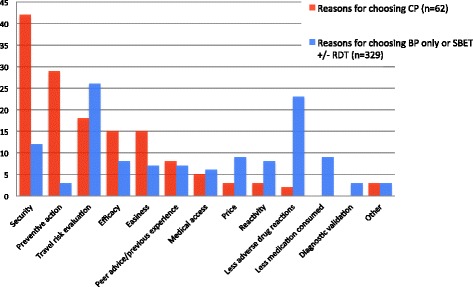
Results: A total of 391 travellers were included from December 2012 to December 2013. Fifty-nine (15%) opted for chemoprophylaxis, 116 (30%) for stand-by emergency treatment, 112 (29%) for stand-by emergency treatment with rapid diagnostic test, 100 (26%) for bite prevention only, and four (1%) for other choices. Travellers choosing chemoprophylaxis justified their choice for security reasons (42%), better preventive action (29%), higher efficacy (15%) and easiness (15%). The reasons for choosing stand-by treatment or bite prevention only were less medication consumed (29%), less adverse drug reactions (23%) and lower price (9%). Those who chose chemoprophylaxis were more likely to have used it in the past (OR = 3.0 (CI 1.7-5.44)), but were not different in terms of demographic, travel characteristics or risk behaviour.
Conclusions: When travelling to moderate- to low-risk malaria areas, 85% of interviewees chose not to take chemoprophylaxis as malaria prevention, although most guidelines recommend it. They had coherent reasons for their choice. New recommendations should include shared decision-making to take into account travellers' preferences.
Figures
References
-
- WHO . World Malaria Report 2011. Geneva: World Health Organization; 2011.
-
- Lars R. Who needs drug prophylaxis against malaria? My peronal view. J Travel Med. 2005;12:217–21. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
