

Systematic review and meta-analysis of totally laparoscopic versus laparoscopic assisted distal gastrectomy for gastric cancer
- PMID: 25889971
- PMCID: PMC4384388
- DOI: 10.1186/s12957-015-0532-7
Systematic review and meta-analysis of totally laparoscopic versus laparoscopic assisted distal gastrectomy for gastric cancer
Abstract
Background: Totally laparoscopic distal gastrectomy (TLDG) has been developed in the hope of improving surgical quality and overcoming the limitations of conventional laparoscopic assisted distal gastrectomy (LADG) for gastric cancer. The aim of this study was to determine the extent of evidence in support of these ideals.
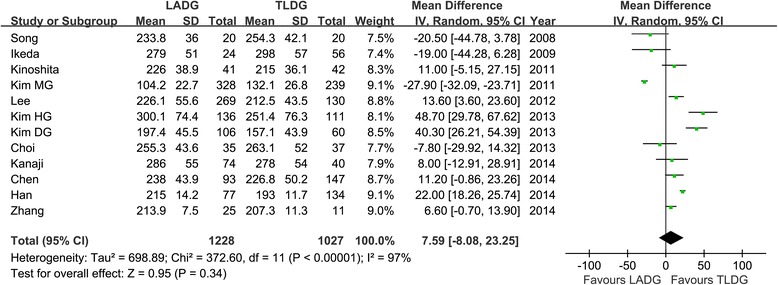
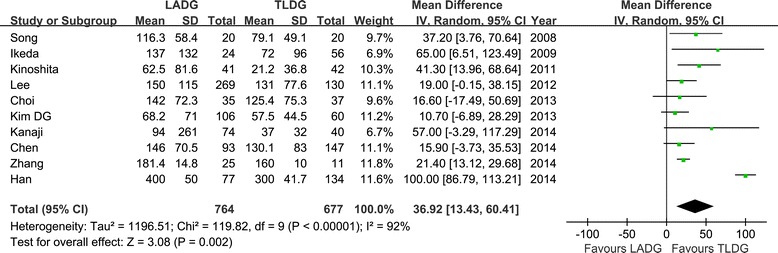
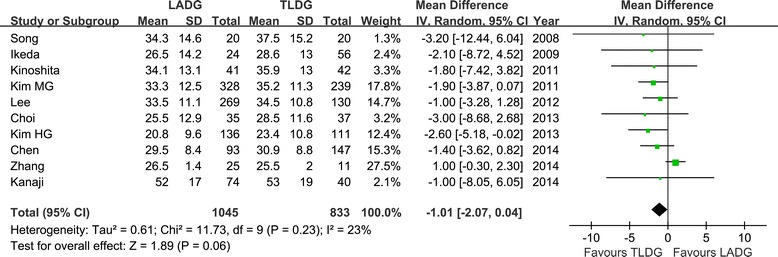
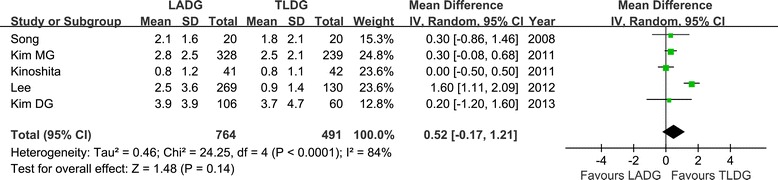
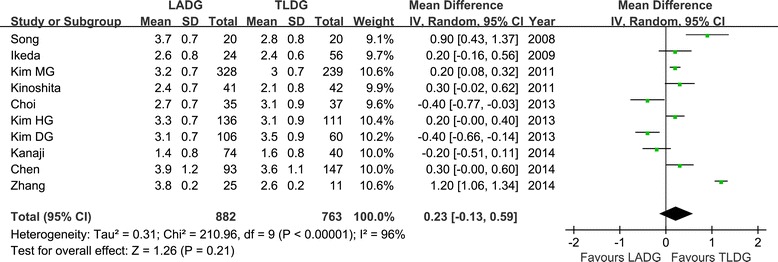
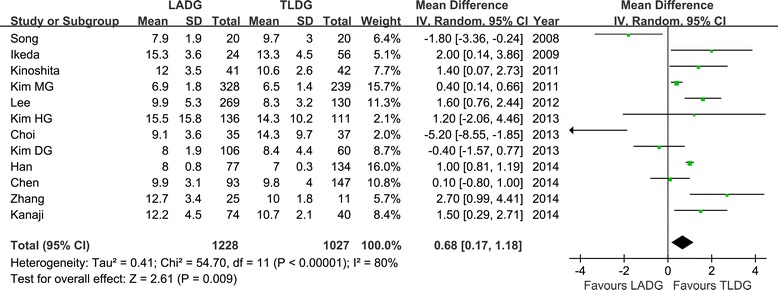
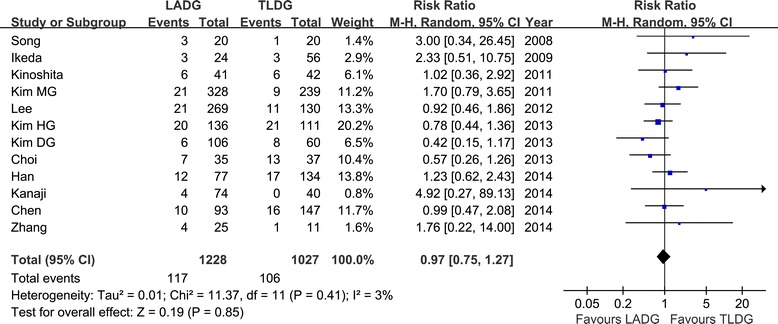
Methods: A systematic review of the two operation types (LADG and TLDG) was carried out to evaluate short-term outcomes including duration of operation, retrieved lymph nodes, estimated blood loss, resection margin status, technical postoperative complications, and hospital stay.
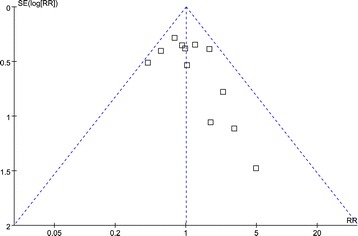
Results: Twelve non-randomized observational clinical studies involving 2,255 patients satisfied the eligibility criteria. Operative time was not statistically different between groups (P > 0.05). The number of retrieved lymph nodes and the resection margin length in TLDG were comparable with those in LADG. Estimated blood loss was significantly less in TLDG than that in LAG (P < 0.01). Compared to LADG, TLDG also involved lesser postoperative hospital stay (P < 0.01) and earlier time to soft diet intake (P < 0.05). Time to flatus and postoperative complications were similar for those two operative approaches.
Conclusions: TLDG may be a technically safe, feasible, and favorable approach in terms of better cosmesis, less blood loss, and faster recovery compared with LADG.
Figures
References
-
- Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4:146–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
