

The cost of hospital-acquired complications for older people with and without dementia; a retrospective cohort study
- PMID: 25890030
- PMCID: PMC4376999
- DOI: 10.1186/s12913-015-0743-1
The cost of hospital-acquired complications for older people with and without dementia; a retrospective cohort study
Abstract
Background: Increased length of stay and high rates of adverse clinical events in hospitalised patients with dementia is stimulating interest and debate about which costs may be associated and potentially avoided within this population.
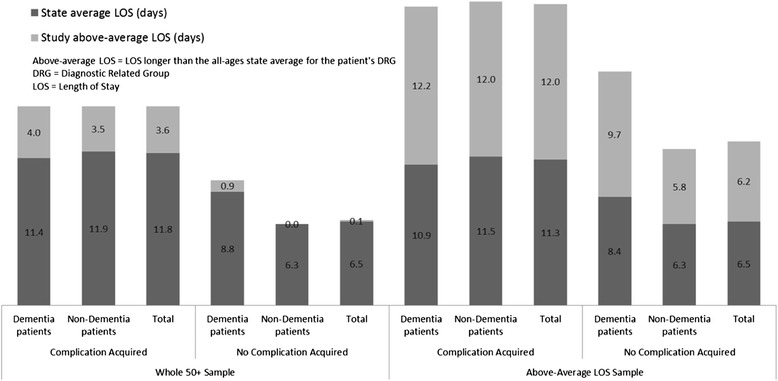
Methods: A retrospective cohort study was designed to identify and compare estimated costs for older people in relation to hospital-acquired complications and dementia. Australia's most populous state provided a census sample of 426,276 discharged overnight public hospital episodes for patients aged 50+ in the 2006-07 financial year. Four common hospital-acquired complications (urinary tract infections, pressure areas, pneumonia, and delirium) were risk-adjusted at the episode level. Extra costs were attributed to patient length of stay above the average for each patient's Diagnosis Related Group, with separate identification of fixed and variable costs (all in Australian dollars).
Results: These four complications were found to be associated with 6.4% of the total estimated cost of hospital episodes for people over 50 (A$226million/A$3.5billion), and 24.7% of the estimated extra cost of above-average length of stay spent in hospital for older patients (A$226million/A$914million). Dementia patients were more likely than non-dementia patients to have complications (RR 2.5, p <0.001) and these complications comprised 22.0% of the extra costs (A$49million/A$226million), despite only accounting for 10.4% of the hospital episodes (44,488/426,276). For both dementia and non-dementia patients, the complications were associated with an eightfold increase in length of stay (813%, or 3.6 days/0.4 days) and doubled the increased estimated mean episode cost (199%, or A$16,403/A$8,240).
Conclusion: Urinary tract infections, pressure areas, pneumonia and delirium are potentially preventable hospital-acquired complications. This study shows that they produce a burdensome financial cost and reveals that they are very important in understanding length of stay and costs in older and complex patients. Once a complication occurs, the cost is similar for people with and without dementia. However, they occur more often among dementia patients. Advances in models of care, nurse skill-mix and healthy work environments show promise in prevention of these complications for dementia and non-dementia patients.
Figures

References
-
- Australian Institute of Health and Welfare. Australian hospital statistics 2011–12, vol. Health Services Series no. 50. Cat. no. HSE 134. Canberra: AIHW; 2013.
-
- Rowell D, Nghiem HS, Jorm C, Jackson TJ. How different are complications that affect the older adult inpatient? Qual Safety Health Care. 2010;19(6):e34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
