

Relation of perioperative elevation of troponin to long-term mortality after orthopedic surgery
- PMID: 25890628
- PMCID: PMC5568001
- DOI: 10.1016/j.amjcard.2015.03.003
Relation of perioperative elevation of troponin to long-term mortality after orthopedic surgery
Abstract
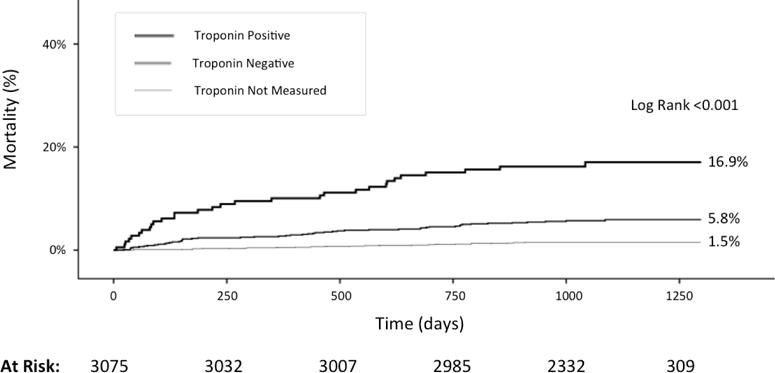
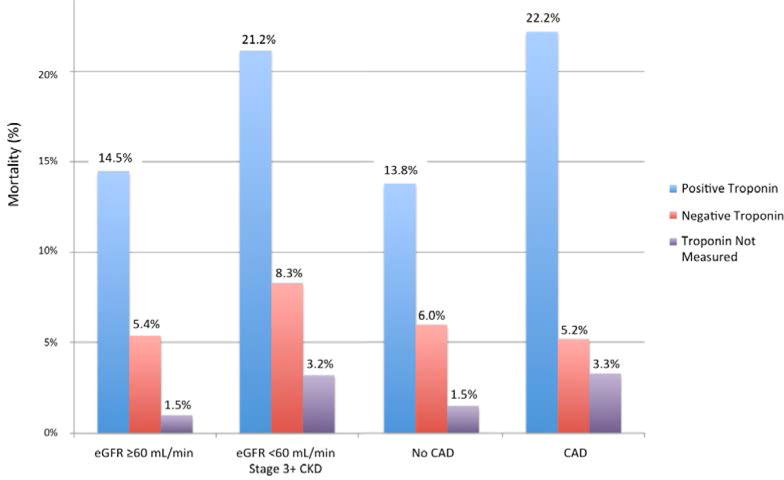
Myocardial necrosis in the perioperative period of noncardiac surgery is associated with short-term mortality, but long-term outcomes have not been characterized. We investigated the association between perioperative troponin elevation and long-term mortality in a retrospective study of consecutive subjects who underwent hip, knee, and spine surgery. Perioperative myocardial necrosis and International Classification of Disease, Ninth Revision-coded myocardial infarction (MI) were recorded. Long-term survival was assessed using the Social Security Death Index database. Logistic regression models were used to identify independent predictors of long-term mortality. A total of 3,050 subjects underwent surgery. Mean age was 60.8 years, and 59% were women. Postoperative troponin was measured in 1,055 subjects (34.6%). Myocardial necrosis occurred in 179 cases (5.9%), and MI was coded in 20 (0.7%). Over 9,015 patient-years of follow-up, 111 deaths (3.6%) occurred. Long-term mortality was 16.8% in subjects with myocardial necrosis and 5.8% with a troponin in the normal range. Perioperative troponin elevation (hazard ratio 2.33, 95% confidence interval 1.33 to 4.10) and coded postoperative MI (adjusted hazard ratio 3.51, 95% confidence interval 1.44 to 8.53) were significantly associated with long-term mortality after multivariable adjustment. After excluding patients with coronary artery disease and renal dysfunction, myocardial necrosis remained associated with long-term mortality. In conclusion, postoperative myocardial necrosis is common after orthopedic surgery. Myocardial necrosis is independently associated with long-term mortality at 3 years and may be used to identify patients at higher risk for events who may benefit from aggressive management of cardiovascular risk factors.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Steiner C, Andrews R, Barrett M, Weiss A. HCUP Projections Report # 2012–03. U.S. Agency for Healthcare Research and Quality; 2012. HCUP Projections: Mobility/Orthopedic Procedures 2003 to 2012. Online September 20, 2012. Available: http://www.hcup-us.ahrq.gov/reports/proiections/2012-03.pdf.
-
- Haralson RH, 3rd, Zuckerman JD. Prevalence, health care expenditures, and orthopedic surgery workforce for musculoskeletal conditions. JAMA. 2009 Oct 14;302(14):1586–1587. - PubMed
-
- Weiss AJ, Elixhauseer A. HCUP Statistical Brief #171. Agency for Healthcare Research and Quality; Rockville, MD: Mar, 2014. Trends in Operating Room Procedures in U.S. Hospitals, 2001–2011. - PubMed
-
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol. 2007 Oct 23;50(17):e159–241. - PubMed
-
- Landesberg G, Beattie WS, Mosseri M, Jaffe AS, Alpert JS. Perioperative myocardial infarction. Circulation. 2009 Jun 9;119(22):2936–2944. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
